
The unsustainable growth of the global population needs to be halted through informed voluntary action. Coercive population policies such as those used in China are unacceptable. On the other hand, many millions of women and couples around the world face pro-natalist forms of coercion, such as being forced to give birth to unwanted children, in the absence of contraceptive services and legal abortion. This is a theme we will come back to in this series.
All countries have some population policy, and it can take many forms. But what causes population policies to become coercive, and include forced use of contraception? In this second blog on the topic, we examine policy changes over time in Peru, where coercive sterilization has been documented during a couple of years in the 1990’s.
By Frank Götmark
Our first blog on this topic described coercion in population policies in China and India, including forced abortion and sterilization. Such policies must be condemned. Not only have they caused distress, they have also contributed to making arguments for reduced population growth controversial. We need to make clear what happened, to learn and minimize the risk that these policies come back. Forced use of contraception still apparently occurs in China, and the media have highlighted coercive birth control in Peru. Here we will take a look at policies in Peru, where good knowledge exists: e.g. a study by Raúl Necochea López of the period 1960-90, by Ernesto Vasquez Del Aguila for 1990-2010, a detailed overview by Anna-Britt Coe, and a broader historical book by Necochea from 2014.
Latin America and Catholicism
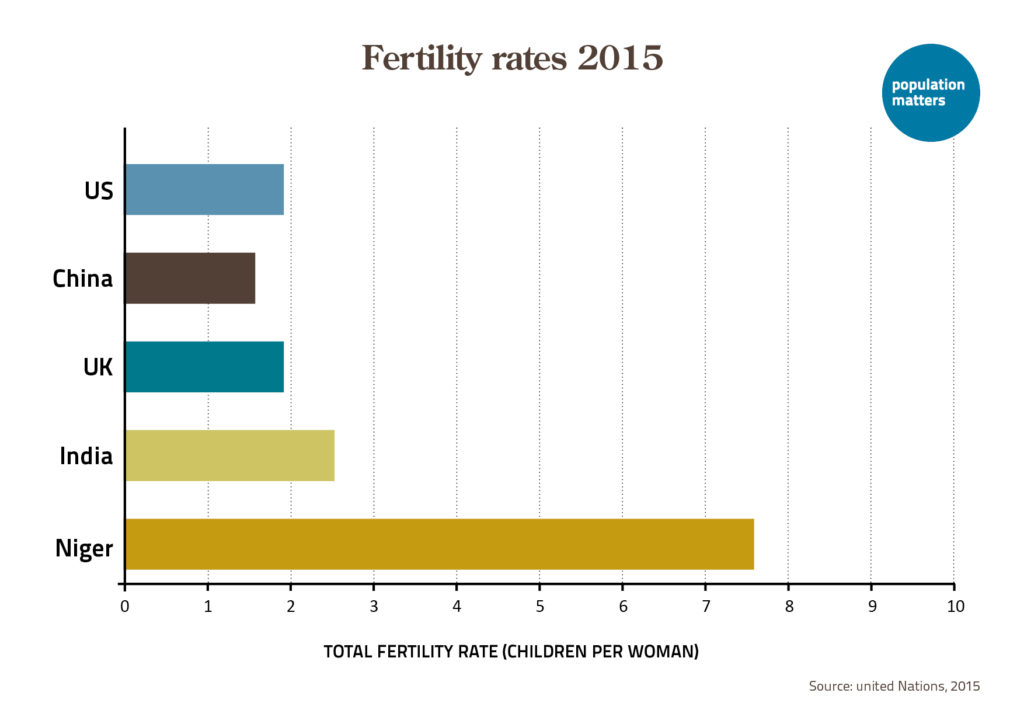
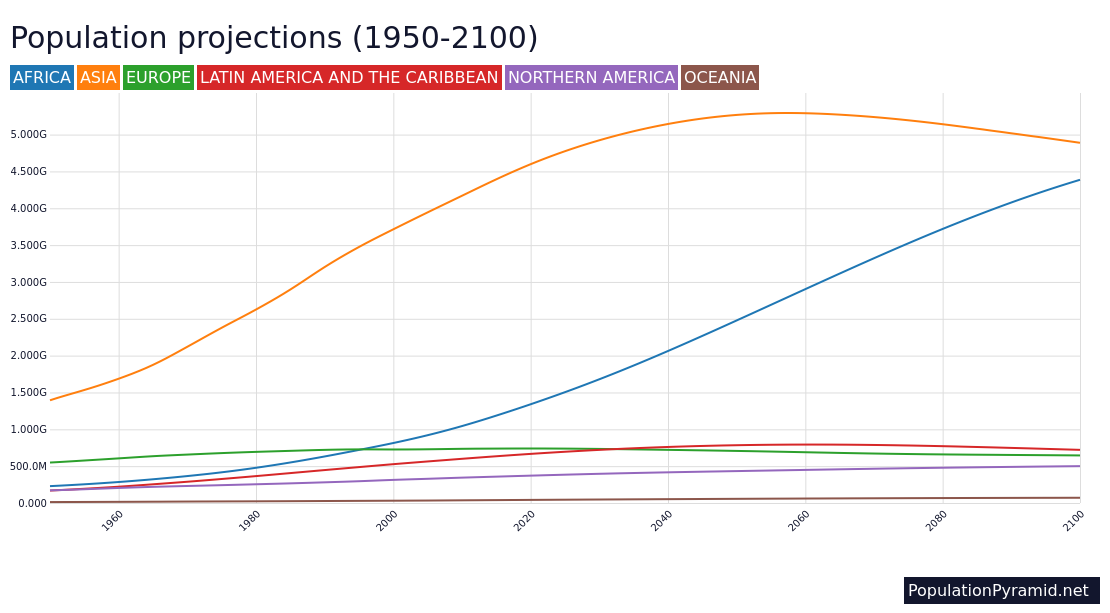
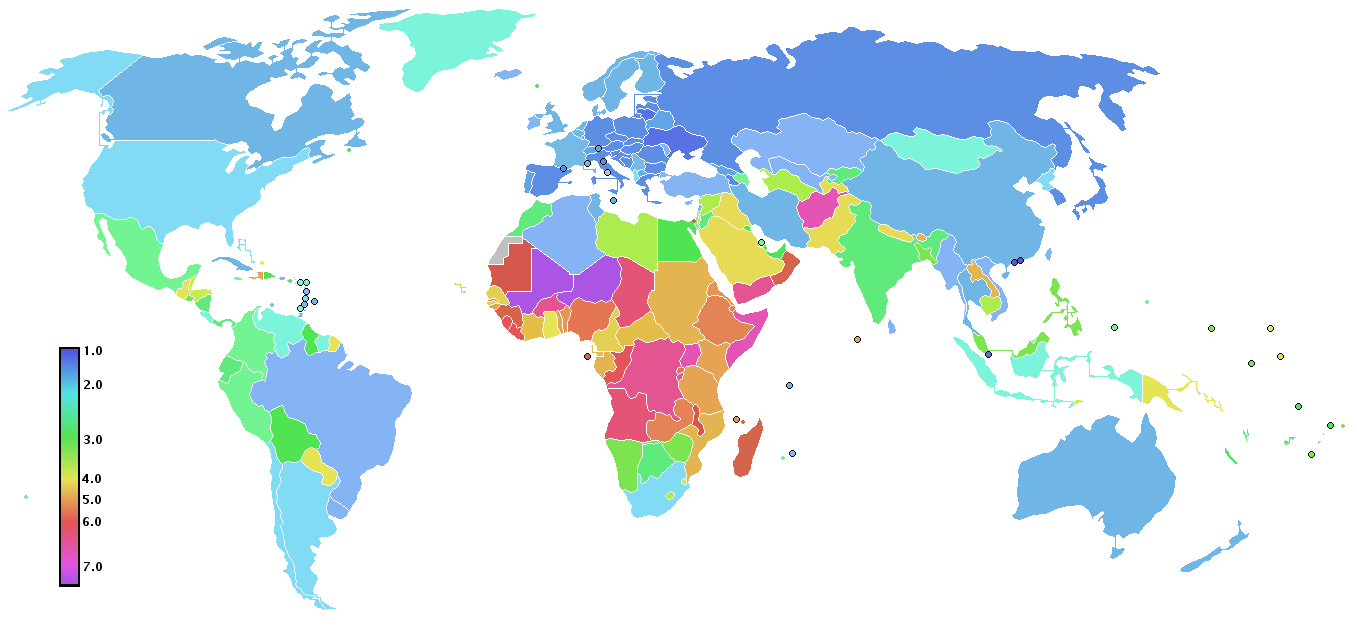
Latin America has intermediate fertility rates, falling in between two categories of western countries with low rates, and Arab States and Sub-Saharan countries with high fertility rates (see our study of global regions). Peru, like all of Latin America, is Christian and dominated by Catholicism. The Vatican long has condemned abortion, accepting only “natural” contraception (e.g., withdrawal, and the rhythm method with abstinence). Necochea’s study of Peru 1960-90 shows how messages from the Vatican were met and modified. Pope Pius XI’s encyclical Casti Connubi from 1930 was the Catholic guideline for contraception up to the late 1960’s. It rejected modern contraception, abortion and eugenics laws that prevented marriage for those deemed unfit. While encouraging mutual love, procreation was the main purpose of sexual relations within marriage, but responsible parents should not have more children than they could care for.
Necochea emphasizes that the Catholic Church, and many priests in Latin America, also followed a social doctrine: the rights and responsibilities of capital and labor, including condemnation of greed through economic power. This was manifested in the “Liberation Theology” that included protests against wealthier capitalist nations draining resources from underdeveloped ones.
Debates on contraception
In February 1968, a Catholic bishop’s conference in Peru acknowledged that fast demographic growth also was a problem. However, the Catholic leaders were worried that foreign agencies, mainly from the US, would influence the government to indiscriminately push birth control on the poor without their consent. In July 1968, Pope Paul VI published the (in)famous encyclical Humanae Vitae that only accepted birth control through natural contraception (the conservative Polish cardinal Karol Wojtyla, the future pope John Paul II, was a main architect of Humanae Vitae). At a conference in Medellin, Colombia in September 1968, Paul VI tried to defend the unpopular text, saying it did not endorse “a blind race towards overpopulation”, and did not forbid “an honest and reasonable limitation of births, nor legitimate medical therapies, or the progress of scientific research”. The conference made clear that population growth in Latin America exacerbated economic and social problems.
In Peru, the first steps to address population growth were taken under Fernando Belaúnde’s presidency (1963-68). Like many other leaders of developing countries, he was educated in the West (France and the US). He created a population agency (CEPD) and in 1966, supported by USAID funding, the government started maternal and family planning clinics. However, Belaúnde’s tenure was interrupted by the leftist military, eager to nationalize oil companies. General Juan Velasco Alvarado, who seized power in October 1968, tried to stop support from US-funded family planning, declaring that development and education would achieve reduced fertility.

A lone pioneer keeps the candle burning
At this time, Dr Joseph Kerrins, an American obstetrician and gynecologist, turned up in Lima. A Catholic charity in New Jersey had provided a contact with the order Sons of Mary. The cardinal Juan Landázuri had asked the Sons of Mary to take over a parish near Lima, and Kerrins designed a program for birth limitation within acceptable Catholic teaching. Necochea cites Kerrins’ observation at the time, for female patients: “there seemed to be no doubt in their minds they wanted me to help them to stop having so many babies”. The contraceptive pill was used, but an educational component was also important. Cardinal Landázuri gave his permission in 1967.
Kerrins, as a US citizen, was warned that his work was sensitive and dangerous in Peru, but directly began working in a clinic that offered gynecological services and voluntary, supervised provision of the pill. On average, 40 women were seeking the pill every day. Soon, by June 1967, there were four more clinics in the surroundings. A crisis arose when Kerrins accepted a grant from a US-based pill provider (Warner Lambert); cardinal Landázuri was angry, but Kerrins managed to appease him. By June 1968, 1200 women were using the pill in eight parish clinics. Of course, Humanae Vitae in July upset Kerrins, as he wondered how would this would affect the program. Yet, according to Necochea, by June 1973 there were 19 parish clinics and more than 5,500 users of the pill. The support of Landázuri, a prominent Catholic in Latin America during 35 years, was important.
By 1976, the program began to decline for political reasons. During 1980-85, Fernando Belaúnde was back as president. Between 1976 and 1988, a new population policy was drafted, and in time it legalized the use of all contraceptives except abortion and sterilization. Foreign donors began financing organizations that offered a broader range of contraceptives.
A new president, a new program
Given the situation in 1990, how could forced sterilization arise, estimated to have affected thousands of women? In 1990, during an economic crisis, amid conflicts and the collapse of several parties, Alberto Fujimori was elected as President. Fujimori, born in 1938, was the son of a Japanese couple that migrated to Peru in 1934. He was educated in Peru as an agricultural engineer, but like Belaúnde also studied during 1964-1969 at universities in France and the US, at a time when the problems of population growth were in focus there. Through a Family Planning (FP) program in 1991, Fujimori tried to strengthen the availability of cost-free contraceptives. He wanted to reduce population growth, fertility, and maternal and child mortality, and simultaneously favor economic growth. Fujimori visited the UN’s Fourth World Congress on Women in Beijing 1995, where FP was emphasized in his talk as follows:
These family planning methods are now legally available in Peru within the reach of women, men, and families of all social classes – so that they can use them, I underline this, freely and responsibly or not use them, if they opt for a different solution according to their personal or family beliefs.

In his talk, Fujimori criticized the Catholic church for trying to prevent the FP program; the church had referred to the program as tied to the “power of darkness”. Politically, Fujimori introduced neoliberal reforms which increased economic growth 1993-95, but this was done under increasing authoritarianism: according to Vasquez Del Aguila he closed Congress and began to rule by decree. Aggressive privatization of public companies also occurred. Moreover, as Anna-Britt Coe makes clear, Fujimori’s early population policy was difficult to get going; the agency in charge of implementation lacked power, and other agencies were not interested. Fujimori also faced violent internal conflict and increasing inflation.
Coercion and its reasons
In September 1995, close to his visit to Beijing, Fujimori and the government included sterilization as part of free contraceptive methods (abortions were still excluded). Coe describes how from this time onwards sexual education expanded, new laws advanced gender equality, and FP clinics obtained more resources. Foreign donors stepped in to support the measures, under a “post-Cairo spirit” (in 1994, the UN’s last population conference was held in Cairo). However, in 1996 the government failed to update the official population policy. Yet, Coe describes how the regime made contraceptive services a core component of a massive poverty relief program. With lower fertility, there would be fewer dependents, and less economic strain in households.
It is at this stage, with a focus on sterilization (mainly tubectomies, fewer vasectomies) that things started to go wrong. Rights to health were emphasized under the Festivales de Salud (“Health Festival”) campaign, but it came to include coercive sterilization. Vasquez Del Aguila and Coe summarize evidence for coercion. In 1996-97, 208 000 sterilizations (10% were vasectomies) occurred, according to official data. The personnel did not have the necessary counselling and medical skills, or equipment. Only 10% of the women are judged to have been sterilized with informed consent, but this percentage is uncertain. The personnel obtained bonuses of U.S.$4 to $10 for each woman brought in for sterilization. There was promotion for “good practitioners”, with threat of losing promotions and incentives if quotas were not fulfilled. Women that underwent sterilization got extra clothing and food. These policies and actions are strikingly similar to those described for India in our first blog (sterilization festivals, food rewards, high targets, bonuses and threats for health-workers who, in turn, threatened persons unless they agreed to be sterilized). In India, vasectomies of men dominated; in Peru tubectomies of women, which are more difficult, and dangerous under unsafe conditions.
Vasquez Del Aguila concludes that justice and reparations are needed for this abuse of human rights. But what other stories are there behind Peru’s FP program? The contraceptives delivered in 1997 included 732 000 IUD’s, pills, injections, condoms and vaginal tablets, far more than the number of sterilizations (Vasquez Del Aguila: Table 1). To judge from Necochea’s work, contraception was welcomed by many women, though the conditions under which FP was offered in the 1970’s favored medical providers’ rather than women’s preferences. Coe states that the violations that occurred in 1996–97 were largely halted by 1998. Sterilizations decreased markedly during 1998-2000, while other contraceptive methods increased (in total almost 3 million users, dominated by pills and injections). In India, coercion involved a minority of clients that used birth control in 1975-77, and this also seems to have been the case for Peru 1996-97. With the new President Alejandro Toledo in 2001 came a backlash against FP programs, just like in India.
Have nations learned from the abuse and mistakes in these FP programs? Reports of coercive sterilizations have come from parts of India as recently as 8-10 years ago. Globally, female sterilization is the most common modern contraceptive method, and more stringent policies for its use may be needed. An experienced obstetrician-gynecologist, Richard Grossman, commented that “although not perfect, IUDs are a wonderful substitute for female sterilization because the failure rate is comparable, less skill is required, it is less expensive, and it is reversible”.
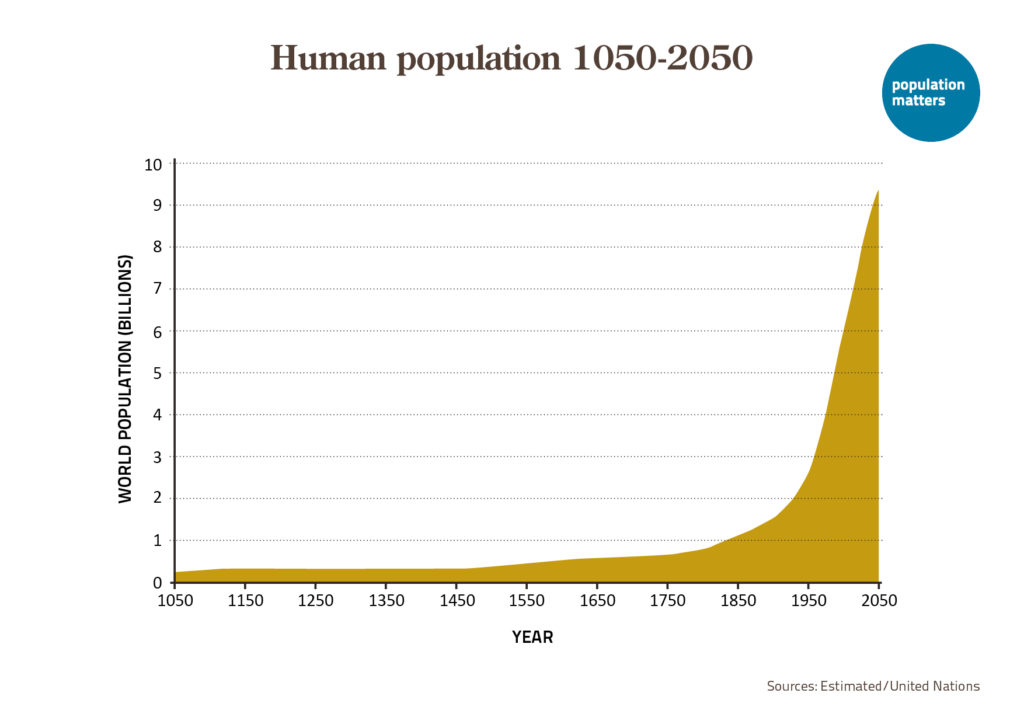
The UN publishes national fertility rates for 5-year periods. In Peru, from 1985-1990 to 2000-2005, fertility fell from 4.2 to 2.7 children per woman (currently 2.2). From 1960 to 2020, Peru’s population increased from 10 to 33 million. Another 8 million are expected before the population peaks. This, combined with strong growth in consumption per capita in Peru and elsewhere, must have affected and will continue to impact the natural resources and wildlife in Peru – a different story, but certainly relevant for a broader picture.
Acknowledgement – I thank Anna-Britt Coe, Richard Grossman, Raúl Necochea, Carl Wahren, and Robert Gillespie for reading and valuable comments.










Leave a Reply