
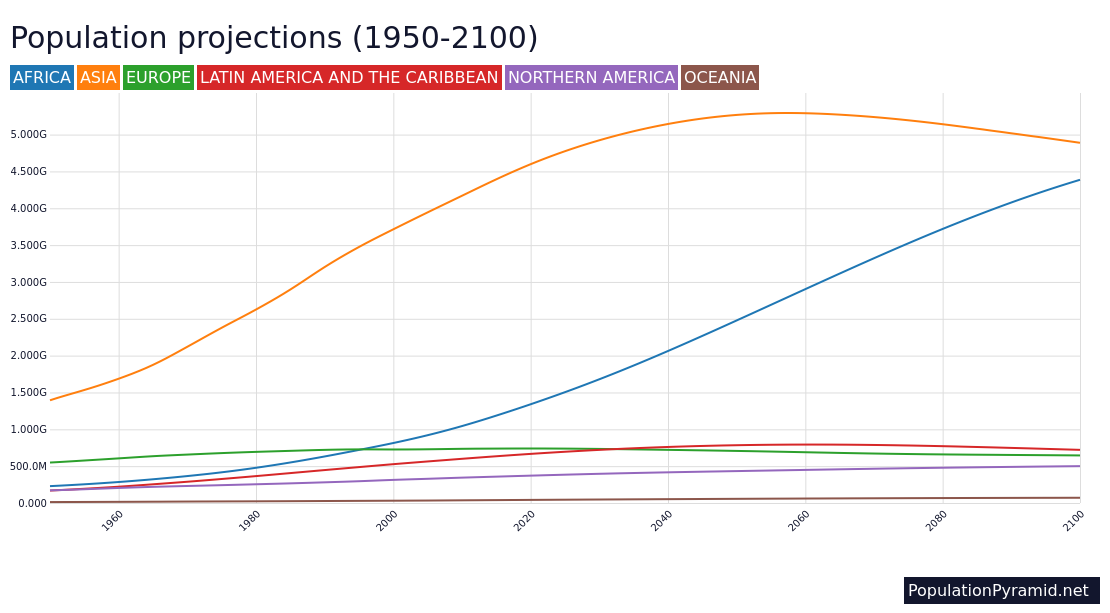
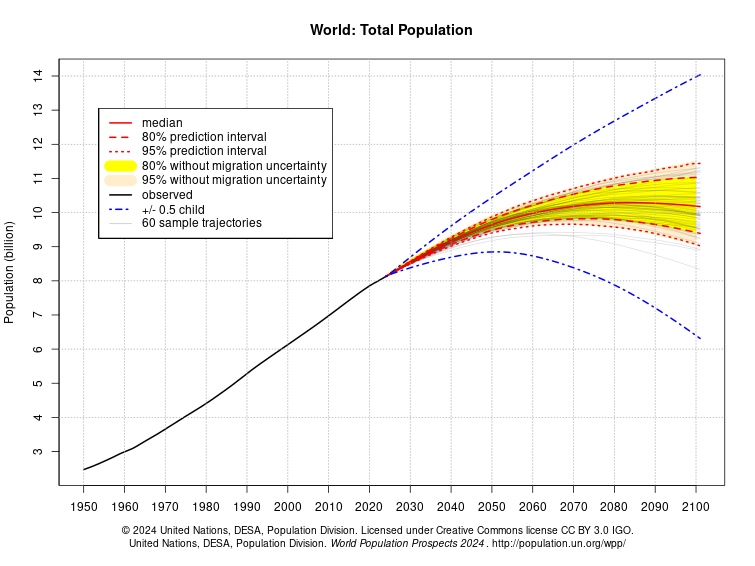
Among the eight regional groups used for the United Nations Sustainable Development Goals (SDGs), only Sub-Saharan Africa (SSA) is projected to sustain a rapid population growth up to 2100, while the seven other regions either have started to decline, or are projected to stabilise, by 21001. In SSA, many countries have a young population; 40-50% of the populations are under 15 years of age, a product of high fertility rates. Population growth in SSA is running at an annual rate of 2.6% as of 20201,2. Although there is variation among the countries, a review of current research suggests broad and consistent differences in fertility rate among followers of different religions.
By Nicola Turner
Religion is a big deal in Sub-Saharan Africa (SSA). Very few people are non-religious according to surveys (only about 1-5%), and studies of that group are rare and unreliable (small datasets). Likewise, little research has examined the effect of religiosity on fertility behaviours. Data on degree of religiosity among individuals are rare, and have only recently become available.
This review draws on 19 quantitative studies from 2010 to 2020, concerning 34 of the 44 countries in continental SSA (for details, see ref. 3). Mostly women were studied, but also men in some studies, in ages spanning 12-65 years. The studies derive data from both national Demographic and Health Surveys (DHS), a standardised survey process overseen by the United Nations and repeated at varying intervals in all SSA countries, and author-devised questionnaires. The religious affiliations examined were African indigenous religions, Christianity and Islam, as well as Catholic and Protestant denominations of Christianity. The authors measured fertility in four ways, as follows (referred to as “fertility” unless specified):
- Children Ever Born (mean number of children, both surviving and dead, who were born alive to all women in a sample)
- Fertility Desires (mean number of children desired)
- Number of Births in Last Five Years (mean number of live births in the last five years)
- Total Fertility Rates (TFR) (average number of children women would bear, if they survived to the end of reproductive life and had the same probability of child-bearing in each age interval as currently prevails across the population)
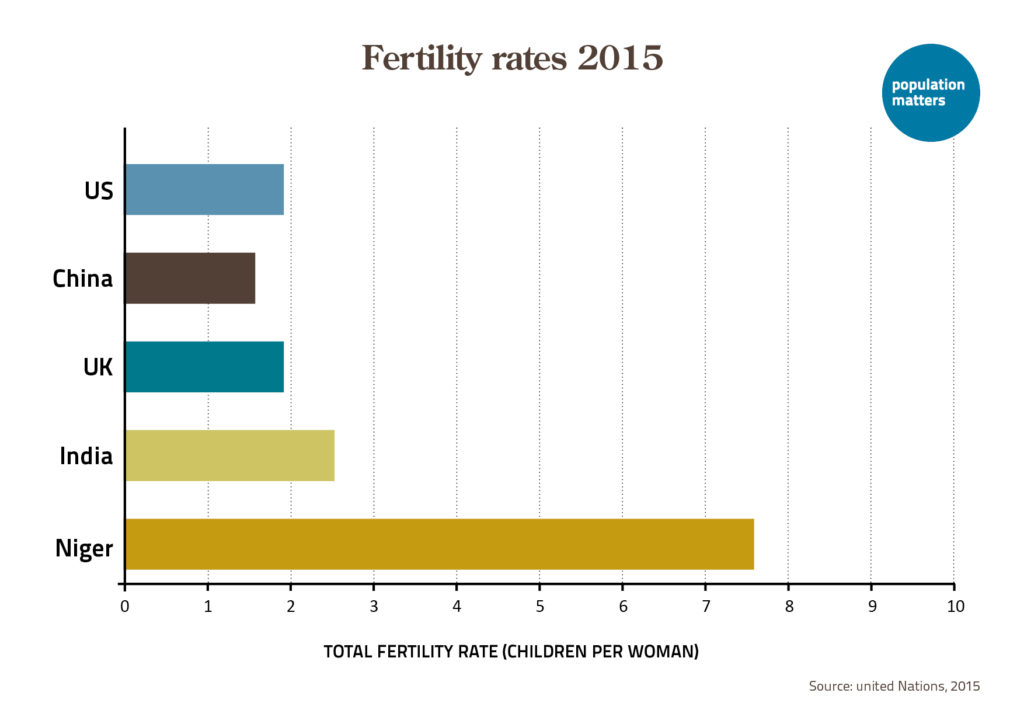
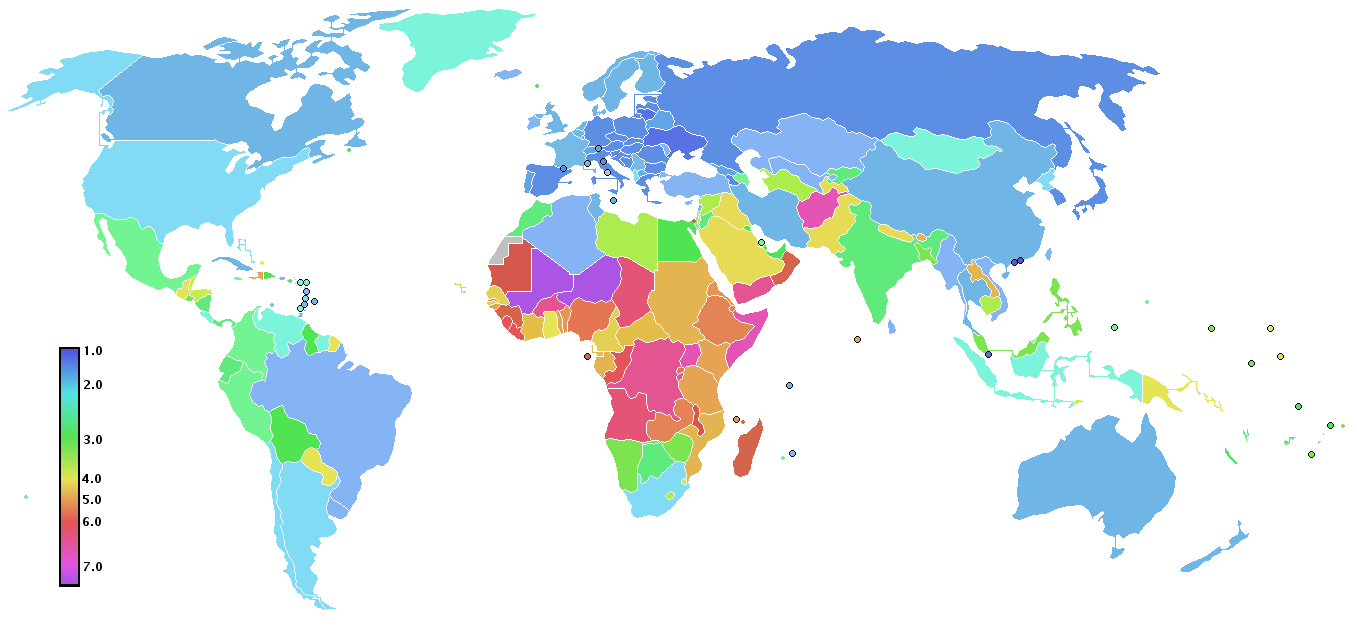
In SSA, TFR values range from 2.2 (Djibouti and South Africa) to 7.0 (Niger). In general, it is lower in Southern Africa (e.g. 2.5 in Botswana, 3.1 in Namibia), and highest in West and Central Africa.
From these studies and measurements, I calculated the magnitude of fertility difference between religions. Figure 1 shows that participants affiliated with African indigenous religions had higher fertility than Christians (all denominations pooled) in all 21 countries that measured fertility for both religious groups. The magnitude of difference was largest in Liberia, but followers of indigenous religions had at least 50% more children than Christians in Sierra Leone, Kenya, Guinea and Zambia. Namibia, Mozambique, Benin, Zimbabwe, Lesotho and Chad had the smallest magnitude of difference between the two religious groups (fertility difference of 10% or less). The average fertility difference between these groups across all countries is 26%.

Of the cluster of countries that had the smallest magnitude of difference in fertility between African indigenous religions and Christianity, two nations – Lesotho and Namibia – belong to the region of Southern Africa. In addition, Zimbabwe is close to this region. In a study by Michel Garenne4, countries in SSA with the highest levels of education were located in predominantly Christian Southern Africa. The percentages of women who had completed primary education in Zimbabwe, Lesotho and Namibia were 78%, 74% and 71%, respectively; the highest in SSA. Although followers of indigenous religions had higher fertility than Christians, fertility for indigenous religion followers was lowest in Southern Africa, indicating a relationship between education (and/or degree of religiosity) and fertility. Sociologist Tim Heaton5 suggests that changes in attitudes and behaviour as a result of socioeconomic changes had a strong influence on Christian groups, especially in countries that are predominantly Christian, which explains the lower fertility observed in these countries.
Figure 2 shows that Muslims have higher fertility than Christians (all denominations pooled) in 25 countries studied. Uganda and Zimbabwe, however, show a weak opposite trend. Gabon displayed the largest magnitude of difference of 36%. Mozambique, Chad, the Central African Republic, Burkina Faso, Ivory Coast, Tanzania and Rwanda had smaller differences, less than 10%. The average fertility difference across all countries is 16%. Thus, these results indicate a difference in fertility between Muslims and Christians, with the latter again having lowest fertility.

Zimbabwe is predominantly Christian and characterised by high levels of education, smaller gap in gender equality and little religious variation. Uganda is also a primarily Christian country with 84.4% of its population identifying as Christian and 13.7% being Muslim1. However, average years of schooling is only 5.4 years (as compared to 9.0 years in Zimbabwe) with only 33% of women having completed primary education4 which may explain why fertility is higher than in Zimbabwe (TFR 5.5 versus 3.9). A study found that poor people in Uganda are more aware of the financial difficulties of having too many children than the middle and richer classes6, and Muslims tended to more often be poor5,7. Furthermore, a higher proportion of Muslims live in urban areas (32%) compared with non-Muslims (18%)8. Those living in urban areas likely have better access to family planning resources. Previous studies in SSA have shown that in urban settings, TFR is lower and Contraceptive Prevalence Rate (CPR) higher than in rural settings9. This likely explains the higher fertility among Christians in Uganda compared with Muslims. The difference in fertility between Christians and Muslims in Uganda and Zimbabwe is small, suggesting that religious affiliation may not play a strong role in these two countries when education and residential setting are taken into account. Note that “religious affiliation” is distinct from “degree of religiosity”.
High fertility in Western, Central and Eastern SSA is associated with polygynous unions in Islam where men are allowed to have up to four wives10. In the Islamic inheritance system, in polygynous marriages, women with more children get a higher share of the husband’s daily earnings and inheritance at death. In focus group discussions and in-depth interviews (see ref. 3), many Muslim women in polygynous marriages described high fertility as a tactic used against competing co-wives to receive more attention and more wealth from husbands. It was also a tactic used to prevent husbands from taking on additional wives as more children means higher financial responsibility for the husband11-15. Although this type of patriarchy is engrained in many SSA societies, it is also preserved by the women when they apply strategies for economic survival where few opportunities exist for women16,17. Hence, in these countries religious differences in fertility levels are stronger. Note also that Muslim populations across SSA are generally poorer and less educated than their Christian counterparts6, indicating unequal economic opportunities.
Fertility differences between Muslims and followers of African indigenous religions (Figure 3) are minor and inconsistent. Muslims had higher fertility in eight countries with the opposite trend in ten countries. Zambia displayed the largest difference of 30% (African indigenous religions having a higher fertility than Muslims). The average fertility difference across all countries is only 2%. Thus, except in Zambia and perhaps Congo, differences in fertility between Muslims and followers of African indigenous religions were small. This can be attributed to the fact that fertility levels were generally high for both religious groups.

Across Christian denominations, fertility among Catholics and Protestants differed little or not at all (Figure 4). Ivory Coast and Lesotho had the largest difference with Catholics having 12% higher fertility than Protestants. All other countries had a fertility difference of less than 10%, and five countries had equal fertility level. The average fertility difference across all countries is 0%. Thus, these results suggest no difference, or small difference in fertility between Catholics and Protestants.

Studies across Western Europe18,19 and the United States20-23 found that fertility decline among Christians was associated with denominational affiliation up until the 1960s, when fertility differences became more associated with degree of religiosity24-26. More religious people favoured formal marriages rather than cohabitation27 and tended to have higher levels of fertility and lower contraceptive use28-31. In developing countries, particularly in SSA where the demographic transition is still at a relatively early stage, fertility differentials are still associated with religious affiliation. Note that at this stage, degree of religiosity varies between different religious affiliations in contrast to later demographic stages where degree of religiosity varies within religious affiliations.
Fertility differences between Catholics and Protestants were small. Some studies documented higher fertility among Protestants than Catholics32,33, others the opposite34-36. In a 2011 study, Heaton5 observed little difference between the two denominations although limitations of the survey data did not allow him to examine religious variations in the heterogenous “Protestant” category. Some studies of Christian “spirit-type” denominations report that members of e.g. Apostolicism and Zionism have higher fertility than both Catholic and Protestant denominations35,37. The findings vary between and within countries, which may be attributed to level of development and stage of demographic transition.
To summarise, followers of African indigenous religions have higher fertility than Christians in all countries that measured fertility for both religious groups. Muslims have higher fertility than Christians, except in Uganda and Zimbabwe (where they are minority groups) also indicating a difference between these two religions. Differences in fertility between Muslims and followers of indigenous religions were small, and the same holds for Catholics versus Protestants. Although there are clear influences of religious affiliation on fertility, the strength of these trends varies within and across countries, suggesting additional influences of factors such as patriarchy, education, wealth, rural-urban gradient, and degree of religiosity. The levels of family planning effort were not examined in this review, but may also contribute to fertility differences among countries in SSA38. Nevertheless, religious influences are strong enough to be an important consideration for economic planners, aid organisations, policymakers and politicians in their population policies.
I wish to thank Frank Götmark for advice and cooperation in my work on this review.
References
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects 2019: Highlights. (United Nations, 2020).
- Week, J. R. Population: An Introduction to Concepts and Issues (12th Edition). (Wadsworth Publishing, 2015).
- Turner, N. Influence of Religion and Religiosity on Fertility and Contraceptive Use in Continental Sub-Saharan Africa: A Comprehensive Review. University of Gothenburg, 195 pages. (2021). doi:10.31237/osf.io/sezdq
- Garenne, M. DHS Analytical Studies, No. 33: Education and Fertility in Sub-Saharan Africa – A Longitudinal Perspective. (ICF International, 2012).
- Heaton, T. B. Does Religion Influence Fertility in Developing Countries? Population Research and Policy Review 30, 449-465 (2011).
- Muhoza, D. N., Broekhuis, A. & Hooimeijer, P. Variations in Desired Family Size and Excess Fertility in East Africa. International Journal of Population Research (2014).
- Pew Research Centre. The Future of the Global Muslim Population. (Pew Research Centre, 2011).
- Westoff, C. F. & Bietsch, K. DHS Analytical Studies, No. 48: Religion and Reproductive Behaviour in SSA. (ICF International, 2015).
- Canning, D., Raja, S. & Yazbeck, A. S. Africa’s Demographic Transition: Dividend or Disaster? (The World Bank, 2015).
- Pew Research Centre. The World’s Muslims: Religion, Politics and Society. (Pew Research Centre, 2013).
- Audu, B. M., Yahya, S., Geidam, A., Abdussalam, H., Takai, I. & Kyari, O. Polygamy and the Use of Contraceptives. International Journal of Gynecology & Obstetrics 101(1), 88-92 (2008).
- Foley, F. E. In Sickness and in Health: Responding to Disease and Promoting Health in Senegal. Doctoral Dissertation (Michigan State University, 2001).
- Izugbara, C. O., Ezeh, A. C. Women and High Fertility in Islamic Northern Nigeria. Studies in Family Planning 41(3), 193-204 (2010).
- Sinai, I., Omoluabi, E., Jimoh, A. & Jurczynska, K. Unmet Need for Family Planning and Barriers to Contraceptive Use in Kaduna, Nigeria: Culture, Myths and Perceptions. Culture, Health & Sexuality 22(11), 1253-1268 (2019).
- Wilson, E. Reproductive Health Case Study: Senegal. (The Futures Group International, 1997).
- Femininity, K. M. Sexuality and Culture: Patriarchy and Female Subordination in Zimbabwe. (ARSRC, 2006).
- Florence, N. Bukusu (Kenya) Folktales: How Women Perpetuate Patriarchy. International Feminist Journal of Politics 15(3), 370-390 (2013).
- Anderson, B. A. Regional and Cultural Factors in the Decline of Marital Fertility in Western Europe in The Decline of Fertility in Europe (eds. Coale, A. J. & Watkins, S. C.). 293-313 (Princeton University Press; 1986).
- Derosas, R. & van Poppel, F. (eds.) Religion and the Decline of Fertility in the Western World. (Springer, 2006).
- Bouvier, L. F. & Rao, S. L. N. Socioreligious Factors in Fertility Decline. (Ballinger, 1975).
- Freedman, R., Whelpton, P. K. & Campbell, A. A. Family Planning, Sterility and Population Growth. (McGraw-Hill, 1959).
- Gutmann M. P. Denomination and Fertility Decline: The Catholics and Protestants of Gillespie County, Texas. Continuity and Change 5(3), 391-416 (1990).
- Parkerson, D. H. & Parkerson, J. A. “Fewer Children of Greater Spiritual Quality”: Religion and the Decline of Fertility in Nineteenth-Century America. Social Science History 12(1), 49-70 (1988).
- Herold, J. M., Westoff, C. F., Warren, C. W. & Seltzer, J. Catholicism and Fertility in Puerto Rico. American Journal of Public Health 79(9), 1258-1262 (1989).
- Mosher, W. D., Williams, L. B. & Johnson, D. P. Religion and Fertility in the United States: New Patterns. Demography 29(2), 199-214 (1992).
- Westoff, C. F. & Jones, E. F. The End of ‘Catholic’ Fertility. Demography 16(2), 209-217 (1979).
- Berghammer, C. Family Life Trajectories and Religiosity in Austria. European Sociological Review 28(1), 127-144 (2012).
- Brewster, K. L., Cooksey, E. C., Guilkey, D. K. & Rindfuss, R. R. The Changing Impact of Religion on the Sexual and Contraceptive Behavior of Adolescent Women in the United States. Journal of Marriage and the Family 60(2), 493-504 (1998).
- Goldscheider, C. & Mosher, W. D. Patterns of Contraceptive Use in the United States: The Importance of Religious Factors. Studies in Family Planning 22(2), 102-115 (1991).
- Hayford, S. R. & Morgan, S. P. Religiosity and Fertility in the United States: The Role of Fertility Intentions. Social Forces 86(3), 1163-1188 (2008).
- Zhang L. Religious Affiliation, Religiosity, and Male and Female Fertility. Demographic Research 18(8), 233-262 (2008).
- Adegbola, O. Religion and Reproduction of Sub-Saharan Africa. African Population Conference (1988).
- Berhanu, B. Religion Fertility Differentials in Shewa, Central Ethiopia. Journal of Family Welfare 40(1), 22-29 (1994).
- Adedokun, L. A. National Survey of Fertility and Family Planning, Phase 1, Southwest Nigeria. 40-41 (Demographic Statistical Survey (DSS) Monograph No. 1 [1973-1975], 1979).
- Agadjanian, V. & Yabiku, S. T. Religious Affiliation and Fertility in a Sub-Saharan Context: Dynamic and Lifetime Perspectives. Population Research and Policy Review 33, 673-691 (2014).
- Chemhaka, G. B. & Odimegwu, C. Individual and Community Factors Associated with Lifetime Fertility in Eswatini: An Application of the Easterlin-Crimmins Model. Journal of Population Research 37, 291-322 (2020).
- Gregson, S., Zhuwau, T., Anderson, R. A. & Chandiwana, S. K. Apostles and Zionists: The Influence of Religion on Demographic Change in Rural Zimbabwe. Population Studies 53(2), 179-193 (1999).
- Bongaarts, J. & Hardee, K. Trends in Contraceptive Prevalence in Sub-Saharan Africa: The Roles of Family Planning Programs and Education. African Journal of Reproductive Health 23(3), 96-105 (2019).










Leave a Reply