
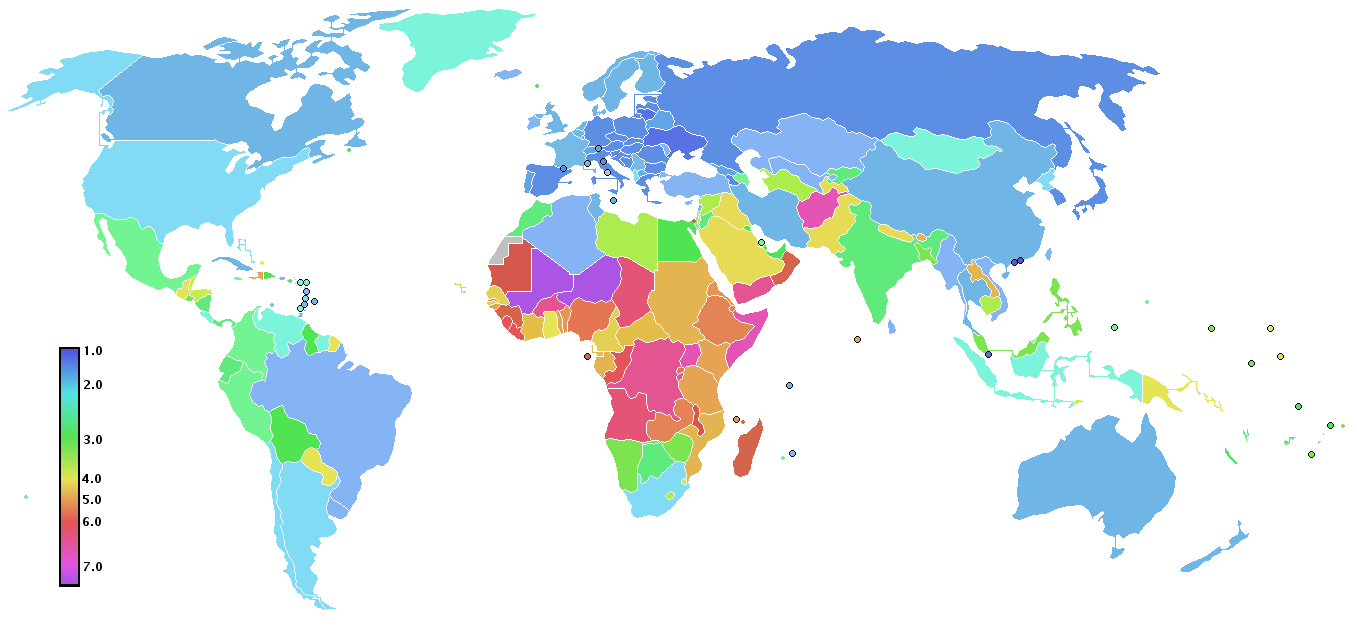
Rwanda has experienced a 40% increase in contraception use within only the past 15 years. The country is located in Sub-Saharan Africa, a region typically known for its high population growth.1 Despite the large rural population, traditional large family norms and strong influence of the religious institutions, Rwanda is slowly becoming known for its efficient, ongoing family planning program.2
By Lili Lantos
 Rural landscape in Rwanda
Rural landscape in Rwanda
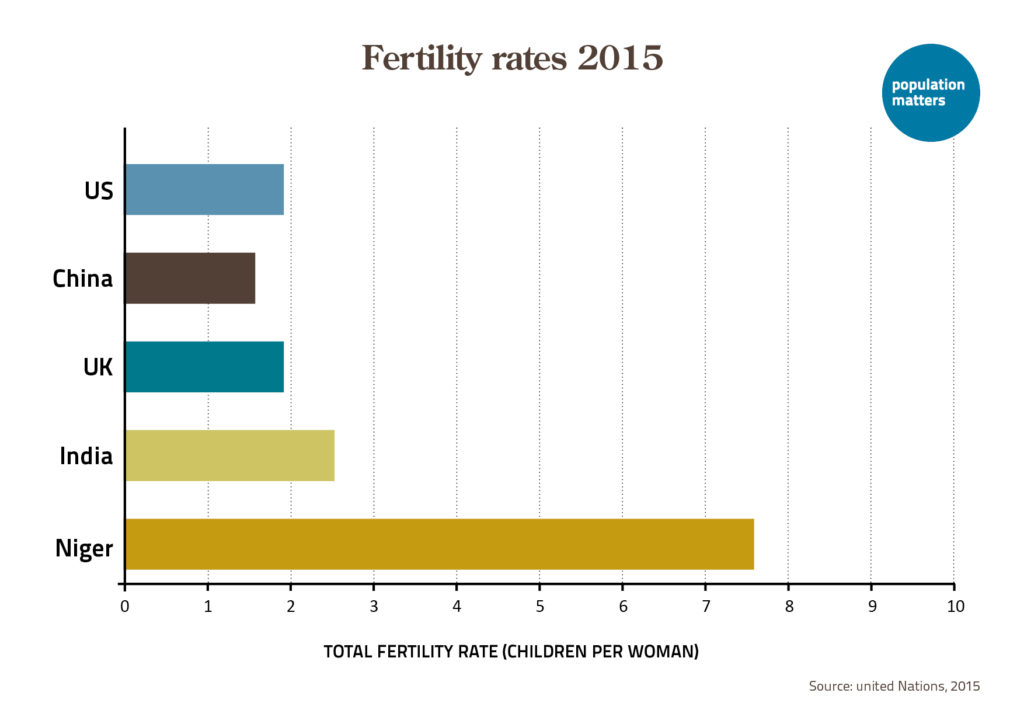
In the 1980s, the average fertility rate for women in Rwanda was between 8 and 8.5 children. This rate decreased to 4 children per woman by 2015, a 50% decrease in 35 years. Strong organisation and implementation facilitated this impressive change, with active political planning and participation being keys to success. When describing Rwanda’s success, the United Nations Population Fund (UNFPA) used the following analogy: “… [for a program to succeed] you need to have 1) a cupboard with all the methods; 2) a chair for the provider—it is not enough to have the method in the cupboard if you do not have a trained provider to offer it; 3) a client motivated to come for services—the services only have meaning if clients come to use them.”
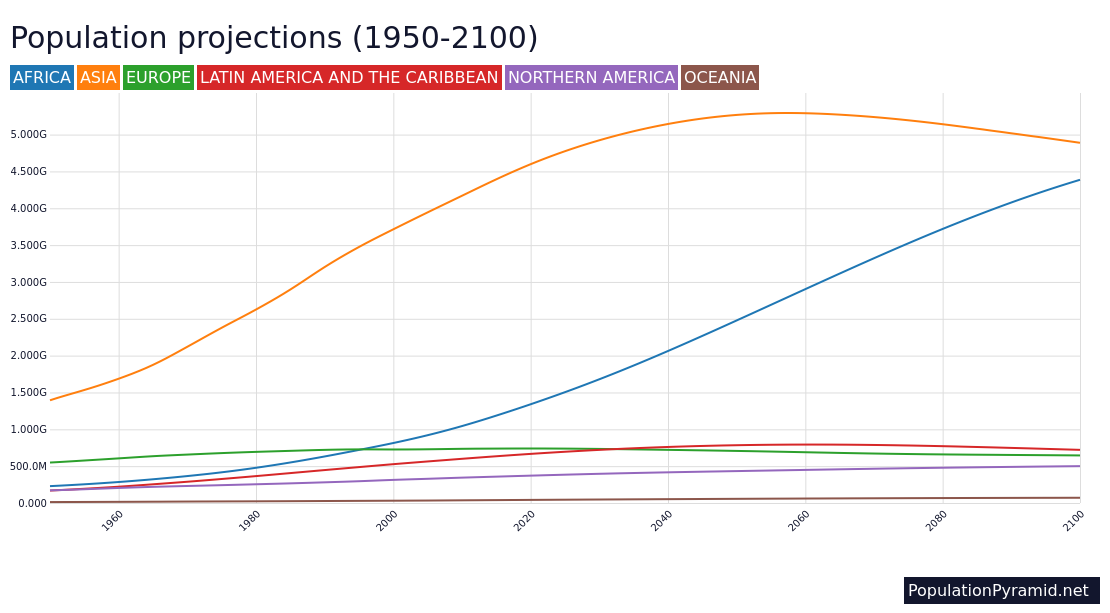
The first Rwandan family planning program was established in 1962, but interrupted due to the 1994 genocide.3 The state is authoritarian and highly centralised, which likely favoured the organised implementation of family planning (FP) programs.3 President Kagame had been holding power since 1994, before being officially elected in 2006, and recently modified the constitution allowing him to be a president until 2034.4 Many human rights activists, opposition candidates, journalists have been attacked or mysteriously died. The definition of poverty has also been changed to present a decline in poverty, when in reality it seems to be increasing.5 Although Rwanda was the first country in the world with a female majority in parliament, it might as well be perceived as a power move by the president, as women in Rwanda have a much weaker role in decision-making as opposed to men. According to the UN (2019) the population of Rwanda is projected to increase from 12.6 million today to 23 million in 2050, and to 33.4 million in 2100 – a serious challenge for such a small country (this projection assumes continuously falling fertility rate). Yet, currently the country has one of the most well-implemented on-going family-planning programs
in Africa.

The centralised power in the country might have helped the FP programs in some ways, as it allowed a quicker and more efficient decision-making process and implementation of the program. On the other hand, the territorial decentralisation of family planning programs was also crucial: a FP program can only be efficient if it provides access to counselling and services for all women and couples through national coverage. This is particularly important in Rwanda, a country where 70% of the population live in rural areas. In 2005, the government implemented a land reform which divided the country into provinces, districts, sectors, cells and health districts, with a plan to introduce ‘one health post at each cell” and provide FP services to as many people as possible.2 In the same year, international financial support strengthened existing government implementations. As a result, between 2005 and 2008, contraceptive use increased from 17,4% to 36,4%. Decentralising the healthcare system also allowed the program to incorporate the needs of different communities in the decision-making process.2
Another key feature of the program was the introduction of community-elected health workers.6 These workers developed close relationships with their communities and were better able to understand community issues and barriers. Equipped with several modern contraceptive methods (short-acting methods, e.g.: condoms, pills, injectables), these health workers became respected by community members and facilitated the acceptance of contraceptive use.2
The Rwandan FP program is funded primarily through international donor organisations: United States Agency for International Development (USAID), Deutsche Gesellschaft für Technische Zusammenarbeit (gtz), Belgian Technical Cooperation (BTC), UNFPA, Department for International Development (DFID) and The William and Flora Hewlett Foundation. According to Solo (2008), USAID planned to spend $500,000 on contraceptives in Rwanda in 2006. This sum reached 2.7 million dollars in 2008, which illustrates the growing demand for FP in the country.2 The main financial donors providing contraceptive procurement areUSAID and UNFPA,and the government is trying to find additional sponsors to create sustainable financing mechanisms for the program.7
The most challenging aspect of the program has been creating the demand for family planning services, as government implementation alone does not guarantee that women and men will decide to reduce their family size. Moreover, with regards to the horrifying 1994 genocide against the Tutsi, the government had to be especially careful when introducing new programs. Solo (2008) identified the importance of the economic status of women in planning their family size, as most of them could not afford having many children. The government decided to communicate the FP program not as a tool to limit the number of children, but to decrease maternal and infant mortality rates. Families were not told to have fewer children; the goal was rephrased to encourage longer time intervals between births, and greater responsibility for each child. In addition, people came to notice the high population density of the small landlocked country, which further motivated participation in the FP program.2
 Young girls carrying water in Rwanda
Young girls carrying water in Rwanda
Altogether, the program’s goal was not only to achieve better health conditions for Rwandan citizens, but also to reduce poverty and encourage economic development. Another aspect of successful implementation was the variety of contraceptive methods offered. The ability to choose between several contraceptive methods further increased the contraceptive prevalence rate (CPR), since the needs of users could be met more easily.2 Despite the high CPR, barriers to contraceptive use remain. As noted by Sempabwa et al. (2006)8, pronatalism is strongly prevalent in the culture and traditions. A 2002 study found that poverty, lack of decision-making power in the family, and religious influence are among the top reasons why women in Rwanda are not using contraceptives.9
Socio-religious factors play an important role in FP program implementations. The Catholic Church owns many health centres in the country, and often challenges family planning goals and implementation.2 However, the influence of the Protestant Church seems to affect FP much more than does Catholicism and lack of education: not using contraception and unmet needs for FP was higher among Protestant women.10 The use of contraception is perceived as a ‘sin’; women who join religious group face a trade-off between being accepted by the community or using family-planning services and contraceptives. Sexual or reproductive health education in the schools is a fairly new thing in Rwanda.12 Talking about sex is still a taboo and young and unmarried women often facing stigma when accessing family planning services.Husbands usually exerting decision-making power, but many of them do not have a good understanding of family planning because they perceived it as a woman’s matter.13 Therefore it is important to highlight the importance of changing social norms.
To conclude, strong political leadership, decentralisation of the healthcare system and introduction of community-based distribution played a major role in the success of Rwanda’s FP program to date. In addition, the relatively fast and efficient implementation also seems to be due to an authoritarian regime, and the power of its executive branch. Six different ministries were involved in the FP program, as well as six international donors. There are still ongoing challenges facing the government, such as finding future donors and changing traditional norms. Although the country should be applauded for the most well implemented ongoing family planning program in Africa, as of 2015, only 12% of women aged 15 to 49 continue to have an unmet need for family planning. Using the current family planning infrastructure as a base, Rwanda should address the remaining barriers to fill this need, as there remains room for improvement.
References:
- Cheikh M. The Persistence of High Fertility in sub‐Saharan Africa: A Comment. Popul Dev Rev. 2017;43(S1):330-337. doi:doi:10.1111/padr.12052
- Julie Solo. Family Planning in Rwanda.; 2008. https://www.intrahealth.org/sites/ihweb/files/attachment-files/fp_in_Rwanda.pdf. Accessed September 18, 2019.
- Löwdin M. The Family Planning Programme in Rwanda : Substantive Representation of Women or Smart Economics? 2017. http://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1174065&dswid=-4427. Accessed September 18, 2019.
- Gatebuke C, Epstein HC. Rwanda’s Elections and the Myth of Women’s Empowerment | The Nation. https://www.thenation.com/article/rwandas-elections-and-the-myth-of-womens-empowerment/. Published 2017. Accessed September 18, 2019.
- Reyntjens F. African Arguments – Lies, damned lies and statistics: Poverty reduction Rwandan-style and how the aid community loves it. 2015. https://africanarguments.org/2015/11/03/lies-damned-lies-and-statistics-poverty-reduction-rwandan-style-and-how-the-aid-community-loves-it/. Accessed September 18, 2019.
- Schwandt HM, Feinberg S, Akotiah A, et al. "Family planning in Rwanda is not seen as population control, but rather as a way to empower the people": examining Rwanda’s success in family planning from the perspective of public and private stakeholders. Contracept Reprod Med. 2018;3:18. doi:10.1186/s40834-018-0072-y
- Government of Rwanda M of H. Rwanda: Family Planning Strategic Plan 2012-2016 | Family Planning 2020.; 2012. http://www.familyplanning2020.org/resources/rwanda-family-planning-strategic-plan-2012-2016. Accessed September 18, 2019.
- Emilaand, Sempabwa; Hoemeke L. Repositioning Family Planning as a Human Right in Post-Genocide Rwanda.APHA Annual Meeting; 2006.
- Africa A. Summary of Findings and Recommendations of Family Planning Qualitative Assessment in Rwanda.; 2002.
- Mahoro J. Unmet need among married women: examining socio-religious influences on family planning use in Rwanda, 2005-2015. Int J Hum Rights Healthc. 2018;11(5):380-391. doi:10.1108/IJHRH-02-2018-0016
- Yeatman SE, Trinitapoli J. Beyond Denomination: The Relationship between Religion and Family Planning in Rural Malawi. Demogr Res. 2008;19(55):1851-1882. doi:10.4054/DemRes.2008.19.55
- UNFPA. UNFPA Rwanda | New curriculum to promote sex education in schools. https://rwanda.unfpa.org/en/news/new-curriculum-promote-sex-education-schools. Published 2016. Accessed September 18, 2019.
- Farmer DB, Berman L, Ryan G, et al. Motivations and Constraints to Family Planning: A Qualitative Study in Rwanda’s Southern Kayonza District. Glob Heal Sci Pract. 2015;3(2):242-254. doi:10.9745/GHSP-D-14-00198










Leave a Reply