
In a world with changing demographic trends, does the retreat by the U.S. government from international population and family planning programs matter? Our answer is a resounding yes.
by Win Brown and Karen Hardee
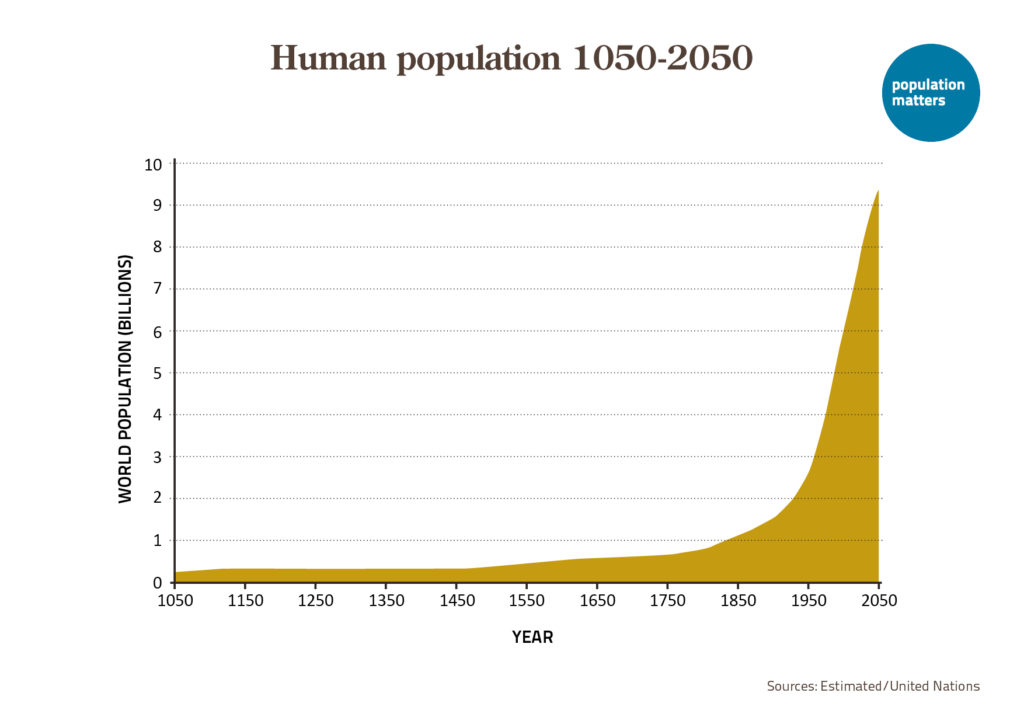
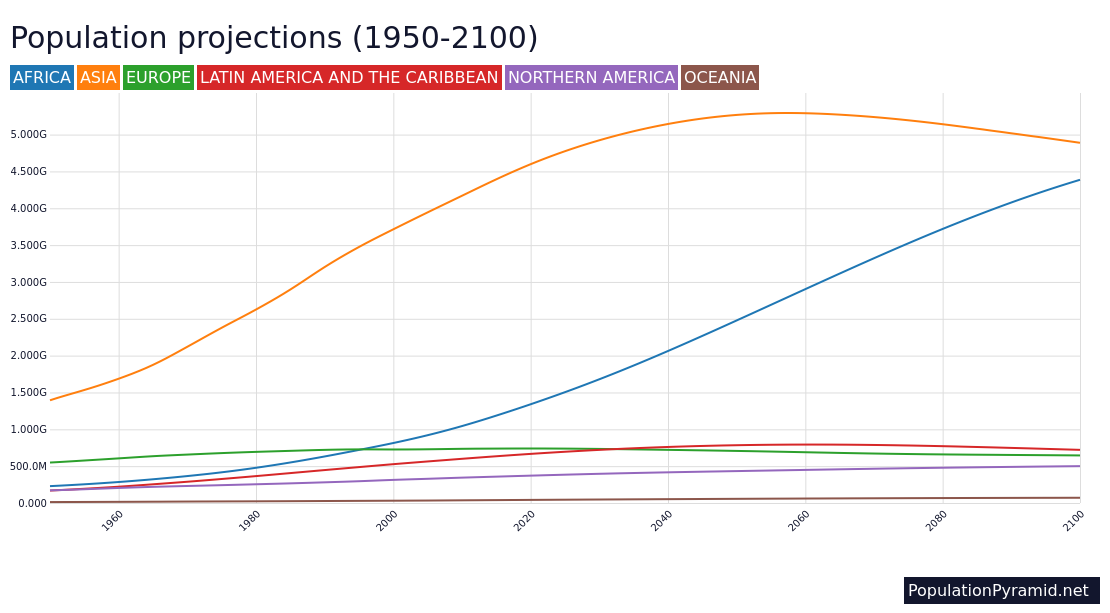
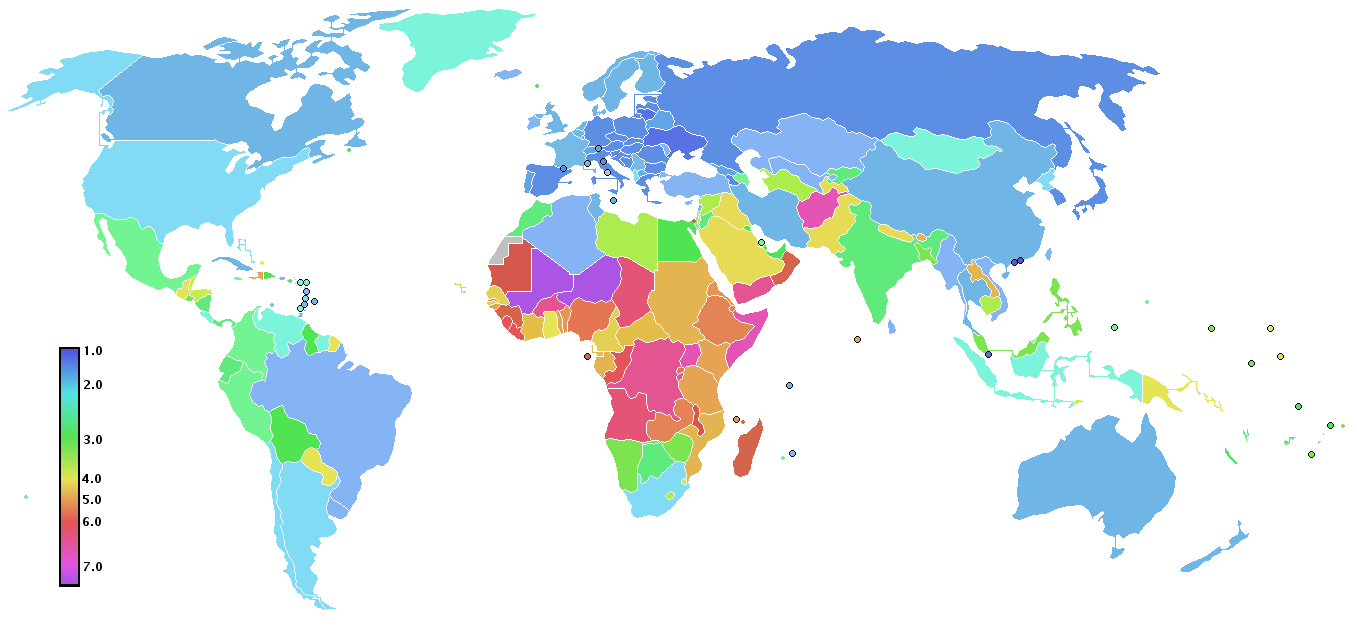
We are demographers who earned our graduate degrees in the 1980s, when academic programs in population and family planning were booming. Back then, concerns about world population were vastly different than they are today. Despite the fact that the overall world population growth rate peaked in 1968, major regions of the world were still experiencing rapid population growth, especially Africa and Asia. The growth was caused by high birth rates. For example, in 1985 the average woman in Africa could expect to bear over 6 children in her lifetime, and her counterpart in South and Southeast Asia could expect to have about 5 children. The scientific and foreign aid establishments of higher-income countries viewed these high birth rates as a threat to global prosperity and environmental sustainability. As a result, we demography students had ample funding.
And so did international family planning (FP) programs. Since the early 1960s, the U.S. government (USG) has been the largest donor to FP and Reproductive Health (RH) efforts around the world. Until Elon Musk took a chainsaw to USAID, the US government was contributing 40% of international assistance for FP/RH (based on 2022 figures – see Figure 1). The high birth rates of the 1980s and 1990s meant that we studied demography during the height of global support for FP/RH programs, which coincided with the height of USG-funded population centers located at universities across the United States, and at similar research institutions all over the world.
Demography is an interdisciplinary field. As social scientists, we were trained to understand the world through a population perspective. We studied the quantitative and qualitative factors contributing to changes in fertility, mortality, and migration. Among the three, fertility was the most prominent focus when we were in graduate school, a trend that has changed over time. As graduate students in the 1980s, we benefited enormously from the scholarship on fertility that flourished in the post-World War II period. We studied birth rates as sociologists, as economists, as anthropologists, as political scientists and historians, and as public health and public policy analysts. Thanks to major projects like the Demographic and Health Surveys (DHS), funded by USAID in collaboration with country governments and other funders such as UNFPA, we demographers were especially adept at using data to explain levels and trends in fertility, between countries and across time periods. We studied fertility at the individual level of a woman living in a poor community, at the country level and everything in between. As a special bonus, we all studied with top students from countries where donors like USAID awarded scholarships. But now Musk and his team have not only cancelled DHS, they have also denied access to existing survey data.
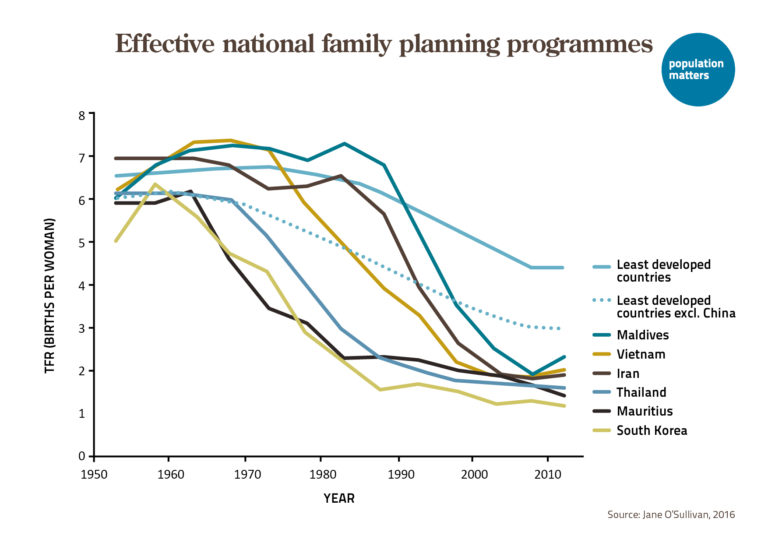
We learned how FP services make a radical difference to women and couples who want fewer children. Across a range of socioeconomic and health indicators, we also learned that countries are better off when family planning services are integrated into the public health system. We analyzed time-series data for countries that had already experienced the aggregate shift from high to low birth rates, learning the characteristic patterns of such fertility transitions. Through internships and then our first jobs in the field, we saw first-hand what success looks like for FP programs, because we spoke to women and men who were able to get access to contraceptive choices for the first time in their lives, and decide for themselves when to have children and how many to have. We spoke with local FP providers who detailed the challenges and best practices of dispensing FP services.
USG support has been very important over the years for what we can legitimately call a global FP success story. Worldwide, spending on FP across all low-income countries is approximately $10 billion each year. Host-country governments typically cover about 75% of the costs. Funds from international donors cover about a quarter of public spending on family planning throughout these countries. This financial and technical assistance from donor nations, especially the United States – and primarily through USAID – has been crucial to the success of FP programs. The reality is that in most countries, family planning programs are not high up on Ministry of Health priority lists. Without the presence of USAID country offices to provide financial and instrumental support to FP and to negotiate cost-sharing arrangements with host governments and other multilateral players, the scope and quality of national FP programs are likely to decline.

The United Nations World Family Planning 2022 reports that globally, out of 1.9 billion women of reproductive age (15-49 years), 874 million are using a modern method of contraception, which corresponds to a modern contraceptive prevalence of 46 percent. The number of modern contraceptive users has nearly doubled worldwide since 1990 (from 467 million). How much impact has the USG had on those numbers? 1965 marks the beginning of USAID’s FP portfolio. At that time, there were fewer than 20 million women using contraceptive methods across the 84 countries where USAID engaged. Today, these countries comprise over 435 million women who currently use contraception, representing over half of all those users estimated by the UN. USAID would never claim sole credit for these numbers, but through its partnerships with governments, private sector leaders, and international organizations, nobody would disagree that USAID was a major facilitator of this “contraceptive revolution.”
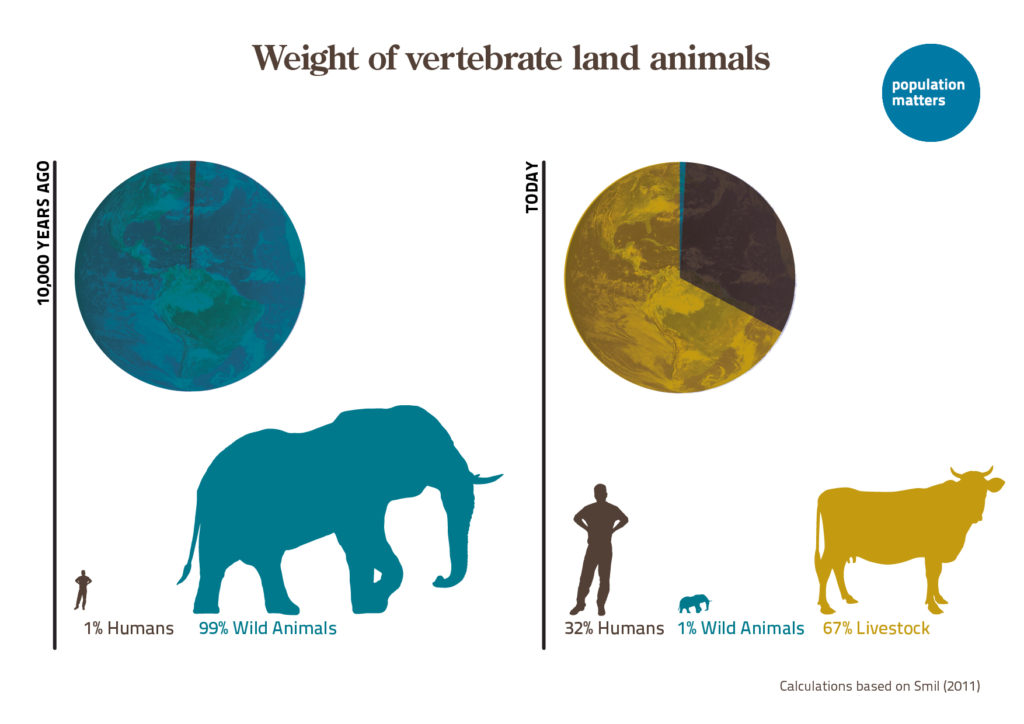
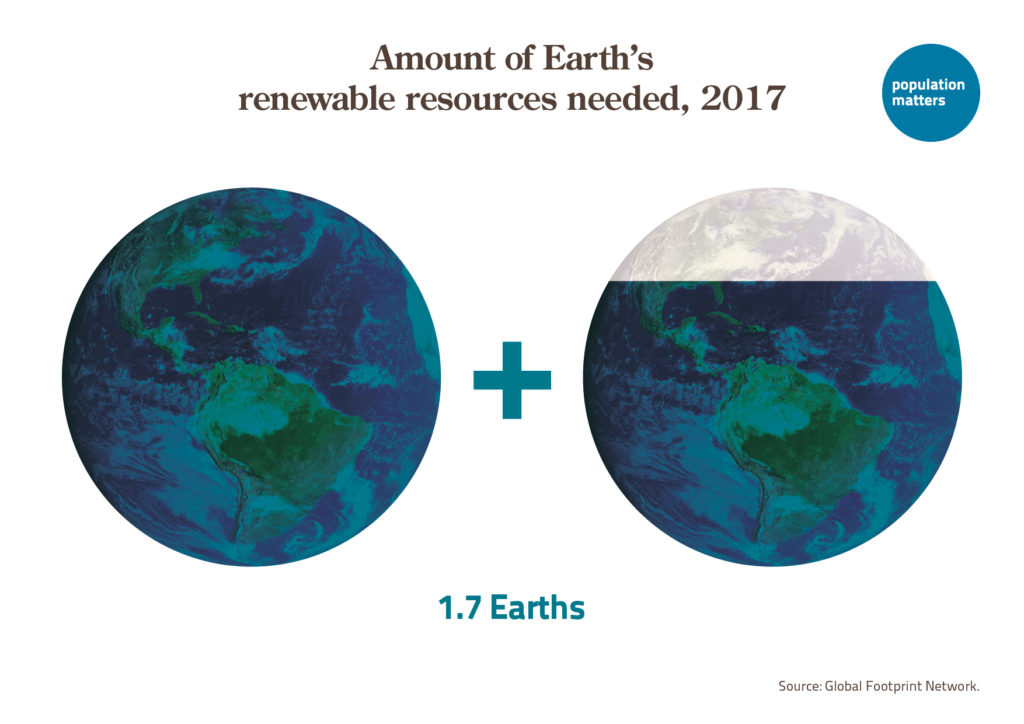
These numbers matter because we know that reductions in fertility from increased use of contraception are correlated with more favorable conditions for socioeconomic development, most notably in the East Asian countries whose economies grew rapidly in the 1970s and 1980s. Since rapid population growth tends to amplify environmental pressures by adding to total economic demand, slowing population growth also implies progress towards a more sustainable future by reducing aggregate demand for food, housing, infrastructure and other services.
At the family level, FP helps reduce high-risk pregnancies that lead to adverse maternal and neonatal outcomes. Fewer pregnancies, especially among the youngest and oldest women, and greater spacing between births also reduce the risk of infant and child mortality. Overall, we would argue that the developmental impact of investing in FP is at the top of the list of foreign aid interventions. Research by the independent Copenhagen Consensus Center named FP a “best buy” for global development, with long-term health and economic benefits worth $120 for each dollar spent on family planning.
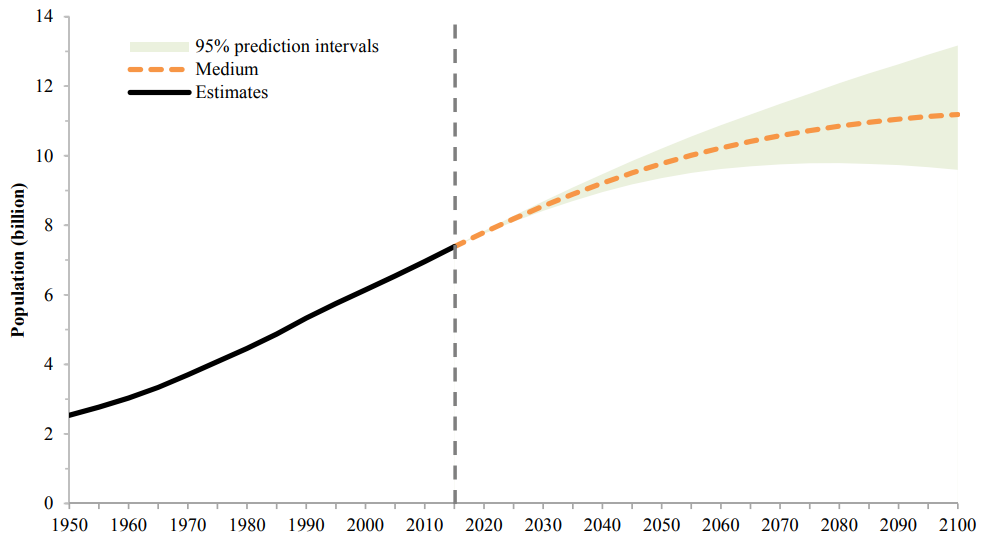
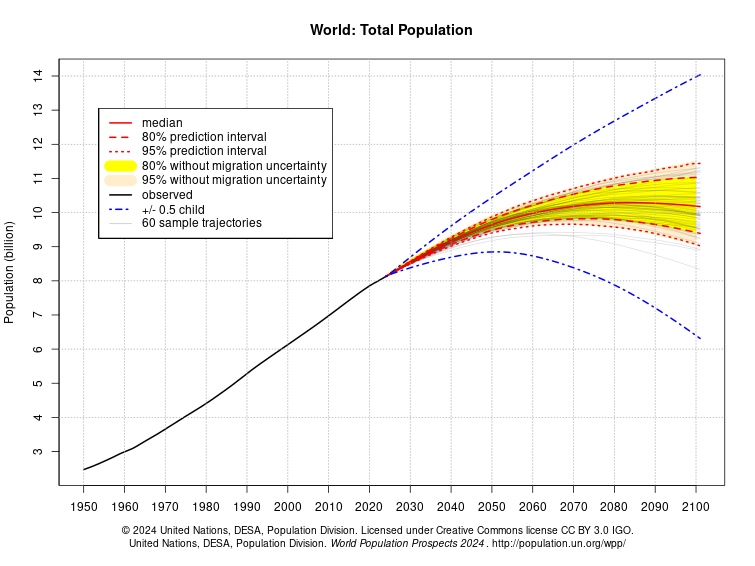
The demography of the world has changed much since we were in graduate school. Parts of the world are characterized by very low fertility, and many politicians are increasingly concerned not about rapid population growth, but rather by rapid population loss. Globally, one in four people lives in a country whose population has peaked, and begun to decline.
These population declines are caused by lower birth rates and in some cases out-migration. The UN reports that women today bear one child fewer, on average, than they did 30 years ago. More than half of all countries and areas globally have fertility below the replacement level of 2.1 live births per woman. This is the level required for a population to maintain a constant size in the long run (without migration) with each generation being followed by another of roughly equal size.
Nearly one fifth of all countries and areas, including China, Italy, the Republic of Korea and Spain, are experiencing “ultra-low” fertility, with fewer than 1.4 live births in the average woman’s lifetime. Further, “by the late 2030s, half of the women in countries with populations that have already peaked will be too old to have children by natural means. Because the share of women in the reproductive age range is projected to decline rapidly in such countries, the impact on population size of policies aimed at raising fertility levels is likely to diminish over time,” according to the UN. Demographers know that once women achieve control over their reproductive lives, there is no going back. Many governments have experimented with policies to spur birth rates, but none has worked.
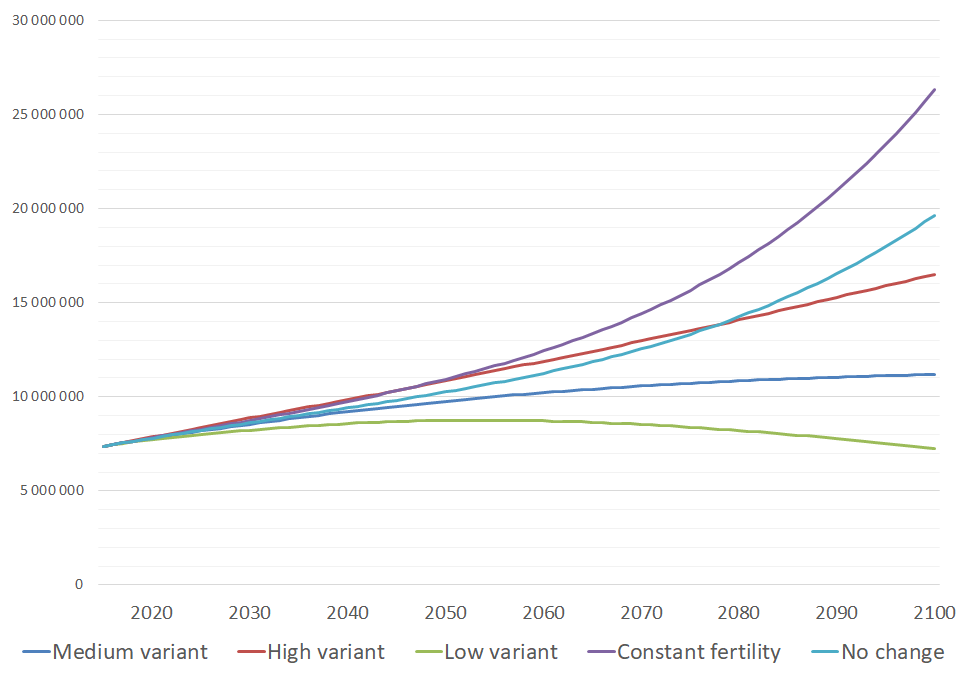
Nevertheless, the global population is still increasing. It is a mistake to believe that FP programs are no longer needed as components of foreign aid. More than 50 African countries have fertility rates over replacement level. Nine countries (India, United States, Indonesia, Pakistan, Nigeria, Ethiopia, Egypt, Democratic Republic of the Congo, and Tanzania) will account for more than half of the increase in global population between now and 2050. Data from now-defunct sources like the DHS suggest that women in most of these countries would prefer to have fewer children. In eradicating USAID and related programs, the United States has ensured that women and couples in these countries will have even less access to quality reproductive health care, with deadly consequences.
Some governments consider their country’s rapid population growth to be a priority policy issue. But these countries have limited capacity to fund FP services. They rely heavily on international aid, in particular on USAID and UNFPA funding that the Trump administration has axed.
Questions about future sustainability are critical for countries like Egypt, where rapid population growth inevitably adds pressure to the increasingly depleted agricultural land in the thin Nile Valley, which competes with the need to build more houses for more people. Special concern should be directed toward a group of countries that are projected to grow exponentially – doubling in size or more – over the next 30 years. These include Angola, Central African Republic, Chad, Democratic Republic of the Congo, Niger, Somalia, and South Sudan. Such rapid population growth in these countries could lead to catastrophic ecological breakdown.
Let’s not forget about the importance of data in this discussion. Demographers are experts on population. We know how populations grow and shrink over time, and the human life implications of doing so, because demographers have built data sources that have been of immense value to policymakers, researchers, and advocates. Defunding a major survey like the DHS – and denying access to existing survey data – rips the heart out of demography, because all of our conversations are punctuated with DHS findings, one way or another. Same for the Census. Do the new power brokers in Washington DC believe they have a better way to collect data? We’ve seen this before: the idea that a big survey is wasteful. That we can monitor population and health trends cheaply, at a distance, e.g., using the tools of Big Data and AI. But we in the field have come to learn that there is no substitute for a face-to-face survey, conducted on the stoop of a real home, with a real person, in a real community. That’s how we interpret data with nuance, and how we ensure that policies are based on evidence that is connected to the people who matter most.

As advocates seek to rescue international assistance from the ashes in the United States, and as other countries contemplate their own foreign assistance, should governments in high-income countries continue to fund international family planning programs and demographic and health surveys? After all, leaders in many high-income countries appear more concerned about depopulation than overpopulation, and more interested in data derived from artificial intelligence than from survey respondents. As signaled above, our answer is a resounding yes.
We need FP programs not just based on developmental and ecological arguments; there is also a moral imperative, as Melinda French Gates articulated in her 2019 book, The Moment of Lift. During her site visits to Gates Foundation projects, she repeatedly heard from women who knew about contraceptives but had no access to them. Listening to their stories convinced her that FP was the fundamental issue: “It hadn’t come as a revelation to me that women want contraceptives. I knew it from my own life, and it was one of the things we supported at the foundation. But after these trips, I began to see it as central, as the first priority for women.”
Supporting less-advantaged countries with something so fundamental to a woman’s life as contraception is not just good science and policy, it is also the right thing to do.
Win Brown, Center for the Study of Demography & Ecology, University of Washington, Seattle. Karen Hardee, Hardee Associates, Washington, DC.










Leave a Reply