
This year marks the 30th anniversary of the United Nations International Conference on Population and Development (ICPD) in Cairo, a watershed event in international population and reproductive health policy. It’s a good time to reflect on its legacy.
by Joseph Speidel and Jane N. O’Sullivan
The ICPD Programme of Action (POA) has served as a policy guide for international action on population and reproductive health since 1994. In response to women’s advocacy, the Cairo meeting featured an increased focus on the rights of women, and called for a wider policy and budgetary emphasis on reproductive health services such as for safe childbirth. The conference also recognized that some past programs had abused reproductive rights in their eagerness to decrease population growth. Hence, language around reproductive rights was strengthened.
In paragraph 7.2 the ICPD calls for:
… the right of men and women to be informed and to have access to safe, effective, affordable and acceptable methods of family planning of their choice, as well as other methods of their choice for regulation of fertility which are not against the law, and the right of access to appropriate health-care services that will enable women to go safely through pregnancy and childbirth and provide couples with the best chance of having a healthy infant.
Abortion
Because UN conference decisions are supposed to be adopted by universal consensus, an enormous share of the discussions at Cairo was taken up by arguments about abortion with the Holy See and some other Catholic countries blocking agreements on language. The Parties, highly committed to producing a consensus statement, went far to appease those who were uncomfortable with or totally opposed to abortion. The conference gave in to abortion opponents and incorporated much language about preventing abortion, asserting that it was not a legitimate activity for family planning programs, and noting that only “In circumstances where abortion is not against the law, such abortion should be safe.” Concessions went no further than encouraging compassionate medical care for women damaged by unsafe abortions.
In the decades since Cairo, those extoling the POA’s call for reproductive rights have overlooked the ICPD’s lack of support for abortion rights. For example:
7.24 Governments should take appropriate steps to help women avoid abortion, which in no case should be promoted as a method of family planning, and in all cases provide for the humane treatment and counselling of women who have had recourse to abortion.
8.25 In no case should abortion be promoted as a method of family planning. All Governments and relevant intergovernmental and non-governmental organizations are urged to strengthen their commitment to women’s health, to deal with the health impact of unsafe abortion as a major public health concern and to reduce the recourse to abortion through expanded and improved family-planning services. Prevention of unwanted pregnancies must always be given the highest priority and every attempt should be made to eliminate the need for abortion. Women who have unwanted pregnancies should have ready access to reliable information and compassionate counselling. Any measures or changes related to abortion within the health system can only be determined at the national or local level according to the national legislative process. In circumstances where abortion is not against the law, such abortion should be safe. In all cases, women should have access to quality services for the management of complications arising from abortion. Post-abortion counselling, education and family-planning services should be offered promptly, which will also help to avoid repeat abortions.
Population
It is also largely forgotten that the Programme of Action clearly affirmed the legitimate threats posed by population growth to poverty reduction and ecological sustainability. The interests of future generations were championed, in 7.3 calling on prospective parents to:
“take into account the needs of their living and future children and their responsibilities towards the community.”
The call was to pursue population stabilisation humanely but in 7.2 warned against targets that can incentivise coercive and involuntary measures.
“Demographic goals, while legitimately the subject of government development strategies, should not be imposed on family planning providers in the form of targets or quotas for the recruitment of clients.”
As we assess the UN’s actions to implement the ICPD POA over 30 years, it seems appropriate to applaud its focus on gender equality, adolescents, and sexual and reproductive health and rights, but also to note that its acknowledgement of the demonstrable value of minimising further population growth was subsequently neglected or denied by the UNFPA. This is linked to the heightened concerns about coercion. Coercive measures had been denounced in earlier international population conferences and the vast majority of family planning programs were free of coercion, but in Cairo the seeds were sown to link demographic goals with coercion. Discussion of population numbers has become taboo and has largely disappeared from UNFPA discourse. Some UN statements go so far as to equate concern about population size and rate of growth with tacit support of coercive, involuntary birth control.
This association is evident in the UNFPA’s 2014 global review of progress under the Cairo Agenda,
“Rapid population growth in the 20th century gave rise to widespread and heavily politicized concerns about overpopulation and the possibility that the world would not be able to generate enough food or other essential resources to sustain its people. The urgent need for the ICPD’s pro-rights platform reflected decades of resulting population and development policies that prioritized population control without heed to people’s reproductive aspirations, their health, or the health of their children.” (p 223)
The statement also dismissed sustainability concerns as politically motivated. A decade later, the UNFPA’s 2023 State of the World Population report focused on the rights of women but was again dismissive of concern about the impact of population size and growth rates on the environment and climate.
“Today, climate change, pandemics, conflicts, mass displacement, economic uncertainty, and other issues fuel concern about over- and under-population. Yet human reproduction is neither the problem nor the solution. (p.5.)
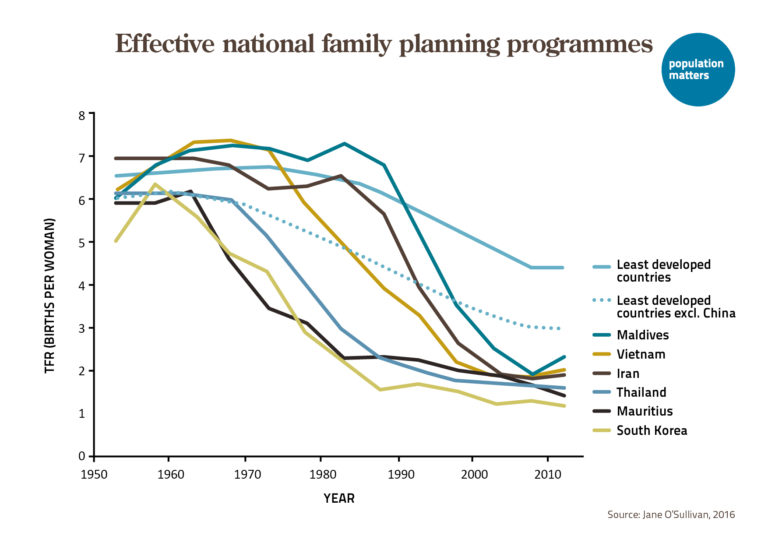
Decades before the ICPD, in many low- and middle-income countries, concern about individual’s reproductive rights, women’s health, lagging economic development and food insecurity provided rationales for implementing national family planning programs. These programs appropriately included messages about the value of small families for the health of mothers and children and for the economic welfare of their families, communities and nations. Family size preferences were addressed through public education, entertainment media, and endorsement by community and religious leaders and peer networks.

With a few unfortunate exceptions, these family planning programs were voluntary and rights-based. They were often integrated with enhanced family health services that greatly benefitted women and girls and made important contributions to national development. The rapid global fertility reduction during the 1970s and 80s was overwhelmingly due to national voluntary family planning programs. It is notable that for decades prior to Cairo major donors, such as USAID and Sweden’s SIDA, worked to ensure that family planning programs were voluntary and explicitly opposed incentives that could be seen as bribes.
So what happened at Cairo? As one wag put it, if you know what happened at Cairo you weren’t there. The current narrative is that the ICPD for the first time introduced concern about women’s reproductive rights and that the earlier focus on demographic goals inevitably undermined those rights. This constitutes revisionist history. It also misrepresents the POA itself.
Funding
Women’s advocacy groups were active and vocal at the conference, but they did not just espouse reproductive rights and seek abandonment of concern about population numbers. Their main ask was a legitimate call for broader programs and increased funding of reproductive health.
A POA innovation was that for the first time a UN conference estimated the cost of their recommendations and suggested a share of one-third from donors and two-thirds from developing countries themselves. It was recognized that the donor share of financial support would need to be much higher in some countries. In contrast to what was known about funding family planning, there was very little data on the cost of implementing reproductive health services. The result was a drastic underestimate of the cost of implementing a broad range of reproductive health activities.
The 1994 ICPD estimated the following funding needs for population programs to be achieved by 2005:
- Family planning: $11.5 billion
- Reproductive health: $5.4 billion
- HIV/AIDS: $1.4 billion
- Basic research and data collection: $0.2 billion
Total: $18.5 billion (in 1993 dollars)
Unfortunately, following the ICPD no additional donor funds were forthcoming and population assistance funding was shifted away from family planning, to support work on HIV/AIDS and other reproductive health activities. As shown in the figure below, the proportion of population assistance provided for family planning declined from over 50% in 1995 to less than 10% in 2008, and funding for family planning declined from $723 million in 1995 to $404 million, figures far short of the $3.8 billion donor share of estimated funding needs (one third of $11.5 billion).

Since 2012, the Family Planning 2020 program and other initiatives have achieved some increase in funding and political commitment to family planning. In 2019, the Guttmacher Institute estimated that increasing expenditures from the then-current $7.1 billion a year to $12.6 billion could satisfy the unmet need for modern contraception in developing countries. If, as called for by the ICPD, donors provided one-third of the $12.6 billion needed, they should be contributing $4.2 billion annually rather than the 2019 figure of $1.52 billion.
Hence, the POA has not met its goal of increasing resources and therefore has fallen short of its goal of improving reproductive health services to women. While the quality of services has increased, the number of women with unmet needs for contraception has grown. Support for SRHR would be strengthened by acknowledging the negative development impacts of population growth, which were formerly a main motivation for governments to support reproductive health services.
Where to from here?
Future goals for international population policy should address the deficiencies of the POA relating to reproductive rights and family planning. A stronger commitment to SRHR should address pervasive gender inequality, incorporate reproductive justice, and foster the rights of the LGBTQIA+ community. It should explicitly recognize that access to abortion information, services, and care is a universal human right.
Other neglected goals of the POA should be addressed, especially adoption of appropriate population and SRHR policies that consider the impacts of rapid population growth on a broad range of issues including health, food security, poverty, the environment and climate. Renewing awareness of the negative impacts of population growth might help elicit adequate funds to ensure that high quality family planning and reproductive health services are available worldwide.
Joseph Speidel is co-author of the new report Breaking Silos: Population and SRHR, thirty years after Cairo.









Leave a Reply