
African researchers have done excellent work to clarify how religious affiliation influences the use of contraception. In Nigeria, with high fertility and a large and growing population, use of modern contraception is still low. The teaching of Islam in particular, contributes to this situation. Several researchers emphasize that men and religious leaders should be involved to improve the situation for women.
By Frank Götmark & Nicola Turner
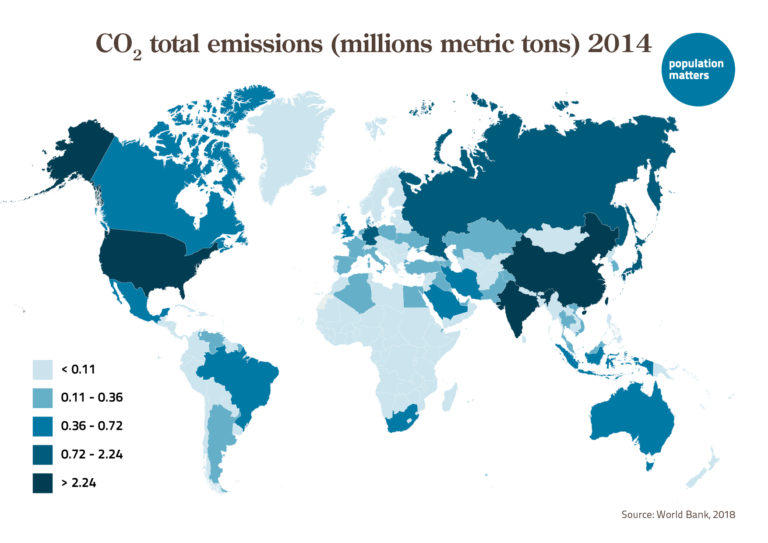
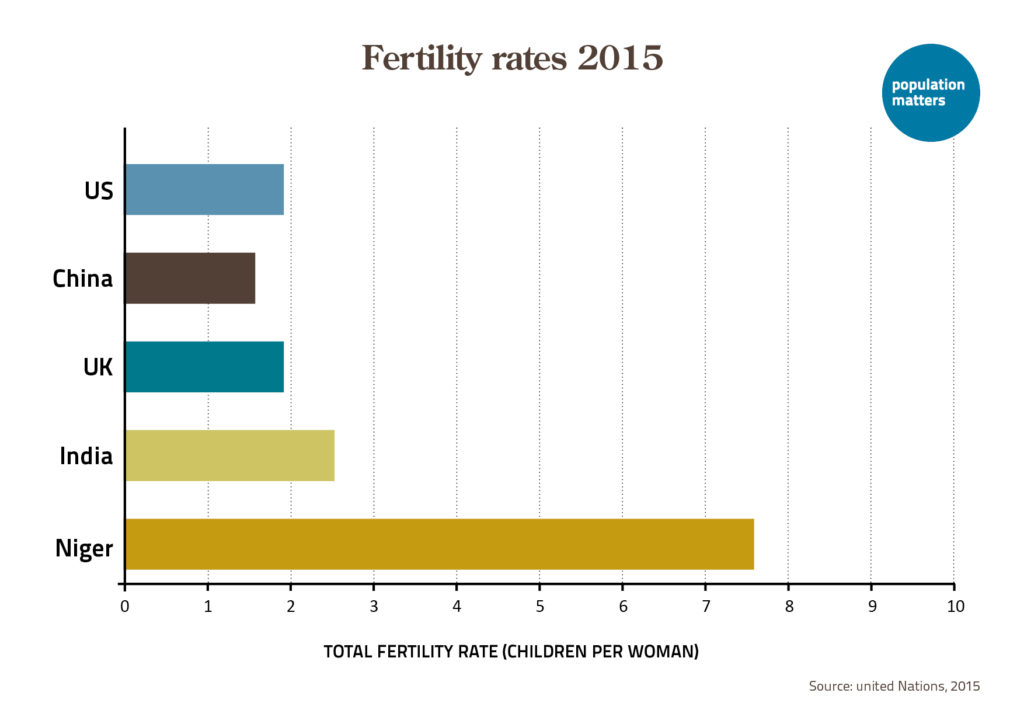
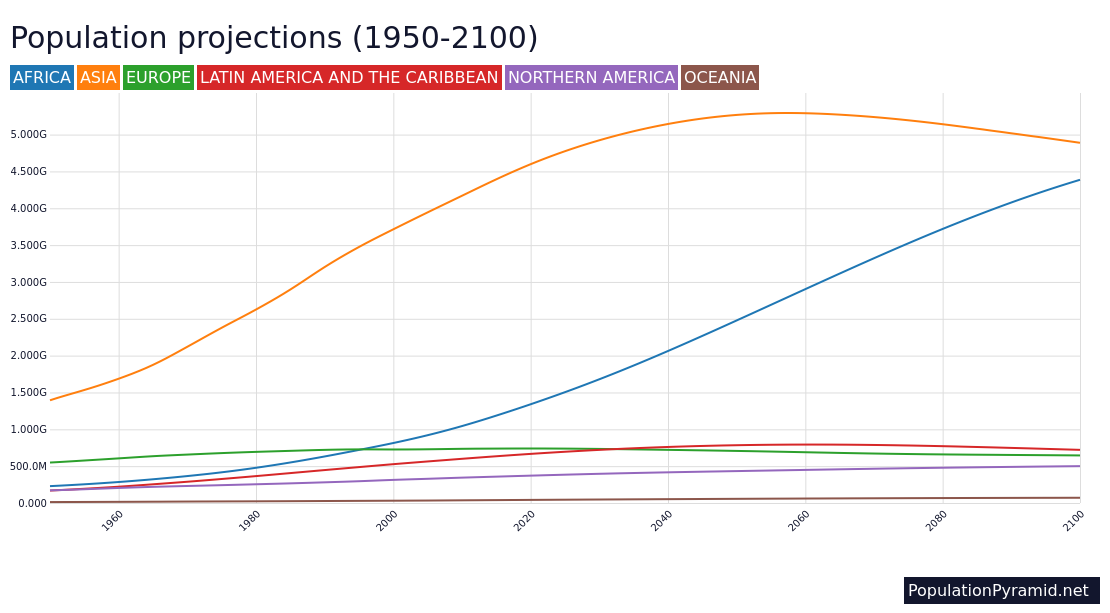
Nigeria, with 211 million people, is projected to have a population of 401 million by mid-2050. This would markedly increase demands of people on water resources, arable land, forests, and wild animals (a food source in rural areas). Today, the number of Nigerians per km2 of arable land (622) is higher than the corresponding figure for Europeans in the EU (448) where population may be stable, or even decreasing. The high fertility rate in Nigeria (5.2 children per woman), combined with a young population forming families in coming decades, seems to be causing a future population explosion. What is the role of religious denominations for this high fertility rate?
African researchers have analyzed the contraception use in Nigeria, and the factors influencing the contraceptive prevalence rate (CPR, the percentage of married women, or in union, using contraception). Demographic and Health Surveys (DHS) are available from many countries in Sub-Saharan Africa (SSA), and can be used to analyze CPR.
In a detailed study, Godswill Osuafor and Akim Mturi asked whether “religious beliefs have a significant effect on contraceptive uptake” in Nigeria. Denomination affiliation is given in the DHS (Catholic, other Christian, Muslim, and traditional religion). Non-religious people were not mentioned, a small, difficult-to-study minority: atheists and agnostics, if open with their views, face persecution in Nigeria and other African countries, or even capital punishment. One wonders therefore, if the proportion of people classified as religious is overestimated in polls from Africa?
Osuafor & Mturi describe the background: The first family planning (FP) clinic was set up in Lagos in 1958, and the first formal FP program began in 1964, with a goal to reduce fertility. A national population policy in 1988 set up specific goals; to reduce the fraction of women bearing more than 4 children by 50% to 1995, and by 80% to 2000. The policy failed; the authors comment that “the benefits of lower fertility… was beyond the comprehension of the ordinary person and even the intellectual.” Both Christians and Muslims in Nigeria tend to view pregnancy as a gift from God. The national population policy was revised in 2004, with goals to reduce the annual population growth rate to 2% or lower, and increasing CPR by at least 2% per year, up through 2015. (In 2019, the annual growth rate was 2.6%, according to the UN.)
Osuafor & Mturi analyzed DHS surveys from 1990, 1999, 2003 and 2008 (the last one involving much more data). The questions to married women (or in union) were the same over time, and the sample of households varied from 5 100 to 23 800. The authors used statistical models to try to tease apart the role of different factors influencing CPR. Such methods should be seen as giving indications, not establishing cause-and-effect, which is only attainable through some form of experiment.
Knowledge of contraception was quite widespread; it increased from 1990 (44% had knowledge) to 2003 (78%), though tended to decline in 2008 (68%). The CPR values were much lower: 6% in 1990, 12% 2003, and 15% in 2008. Knowledge of, and use of contraceptives among Muslims and followers of traditional religion were less than half as high as among Catholic and other Christians (5.6% of Muslims used contraceptives, compared to 19% of Catholics, in 2008). Traditional contraception was the most common method in all denominations across the survey years.
The statistical model, with other factors included or “controlled for”, indicated lower contraceptive use for followers of Islam and traditional religion. Moreover, northern Nigeria had lower CPR than the south, and rural areas had lower CPR than urban areas. Low education and high desire for children were linked to low CPR. In a recent newspaper article, a study by Ekholuenetale and coworkers was quoted for its findings on the influence of religion on contraceptive use; that the predominantly Islamic north had the lowest CPR while Catholics (mainly in the southeast) had the highest.
Osuafor & Mturi explain that the mainly Western funded FP program met resistance, and was called “a Western ploy to reduce Muslims”. It seemed likely that Islam is a negative factor for contraceptive use, independent of other factors. Whether this is true also for Christianity cannot be established without a non-religious reference group. Osuafor & Mturi stated that efforts to increase contraceptive use in Nigeria should target religious leaders, which may be hard in areas where Sharia law and violent Muslim groups (like Boko Haram) seek to eliminate Western influences.
In a second study of the 2013 DHS survey in Nigeria, Ousafor & Ayiga analyzed empowerment of women and education, concluding that education was an important factor for CPR. Of the respondents (representative sample of 16 000 women, aged 15-49), 48% were classified as having “high empowerment”, and 47% had some form of completed education. The proportion of women in rural areas was 66%. Only 6% of the women affiliated with Islam used modern contraceptives. Among Catholics the proportion was 21%, and slightly higher among “other Christians” (26%).
The influence of messages from religious leaders was examined in 2015. A study in Kaduna, Kwara, Oyo and FCT states (map below) showed that the uptake of modern contraceptives was much larger (35%) among women with high exposure to family planning messages from religious leaders (Christians and Muslims), compared to those with medium (24%) or low exposure (14%). The conclusions from this valuable study seem to be robust. According to the Afrobarometer, across 34 African countries, only 46.8% of citizens trust their political leaders, while trust in community leaders, such as traditional (55.8%) and especially religious leaders (69.4%), is much higher (see 2021 Forum report, Mo Ibrahim Foundation).
The latest DHS from 2018, as earlier with much funding from the United States, comprised a representative sample of 41 800 women aged 15-49 (54% followers of Islam). The report is long (700 pp) and rich, but religiosity is neglected (try searching by “religio” in the pdf). Are the religions in Nigeria too controversial for detailed analysis?
In the report, the fertility rate 2015-2017 was 4.5 in urban, and 5.9 in rural areas, and 31% of the women reported that their husband had multiple wives. Moreover, with respect to “ideal family size”, men wanted 7.2 children, and women 6.1 children. The CPR for “any method” among married women was 17%, and for any modern method 12%, up only 2 percentage units from 2013. Remarkably, the CPR of modern method contraceptives by religion is not reported, but for 10 northern Muslim-dominated states, including the large Niger state, it varied from 2-7%; in southerly states, variation was larger (2-29%).
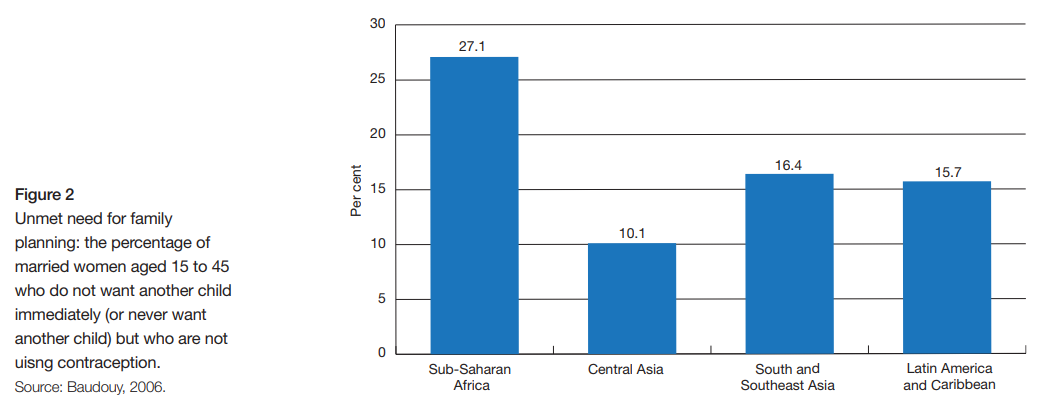
Unmet need for family planning (contraception) among women was studied by nine focus group discussions in Kaduna state, where women expected – not necessarily wanted – to have many children because (1) it is considered their religious duty; (2) men want large families; and (3) increased childbearing wins favor in the competition between wives.
In the northern states, the fertility rate in the DHS 2018 was generally very high (5.8-7.3) while in the southern ones it was lower (see Figure 1). This fertility map can be compared with the population density in Nigeria in 2018 (Figure 2, below).


One study published in 2016 reported that between 1990 and 2013, the fertility of Christians decreased from 6.1 to 4.5, while that of Muslims increased from 6.4 to 6.8. The timing of this change coincides with the institutionalization of Sharia law in 12 northern states in 1999.
The authors projected the change in religious population composition in Nigeria from 2010 to 2060 based on fertility differences in the 2013 DHS, as well as population composition in the absence of fertility difference between religious groups (and also the UN medium scenario assumptions). Assuming constant present 2013 fertility differentials, the Muslim population would increase to a total of 65% of the population in 2060, while Christians would decrease to 32%. With absence of fertility difference, the Christians would only decline from 49.3 to 47.7%, and Muslims increase 1.6%. But if fertility falls more among Christians, and stagnates among Muslims, the latter may constitute 70-80% of the population in 2060.
The authors are careful in pointing out heterogeneity in fertility among Muslims in different states, and suggest that not Islam per se, but the practice of Sharia law in the northern states is a critical factor for high fertility. A broader study from 2015 of 28 countries in SSA found that socioeconomic factors (e.g. education, wealth, gender equality) are not responsible for fertility-related differences between Muslim and non-Muslim women, though in some cases they tend to reduce the difference.
African researchers, like Osuafor & Mtiru and Adedini and coworkers, and in Kenya Abdi & coworkers, conclude that countering the negative notions of family planning requires active engagement of religious leaders, especially Muslim scholars where they are in positions of power at the community level. Melinda Gates, important for the FP2020 program (now FP2030), states in her book about empowering women (“The Moment of Lift” 2021, p. 79) that “Male allies are essential. It’s especially beneficial to have male allies who are religious leaders”. But this was apparently already realized in Nigeria in the 2004 national population policy, which asserted that traditional and religious leaders “are a gateway to social mobilization and community behavior change” (p. 25). In conclusion, much work remains to reduce the strong population growth in Nigeria.
This research is based on the following thesis:
https://thesiscommons.org/sezdq/
Read the rest of the series on religion and fertility in Sub-Saharan Africa:
Part 1: Introduction to studies of religion
Part 2: Differences among denominations
Part 3: A study on Christian denominations in Mozambique









Leave a Reply